

Atherosclerotic coronary lesions with inadequate compensatory enlargement have smaller plaque and vessel volumes: observations with three dimensional intravascular ultrasound in vivo
- PMID: 9538305
- PMCID: PMC1728616
- DOI: 10.1136/hrt.79.2.137
Atherosclerotic coronary lesions with inadequate compensatory enlargement have smaller plaque and vessel volumes: observations with three dimensional intravascular ultrasound in vivo
Abstract
Objective: To compare vessel, lumen, and plaque volumes in atherosclerotic coronary lesions with inadequate compensatory enlargement versus lesions with adequate compensatory enlargement.
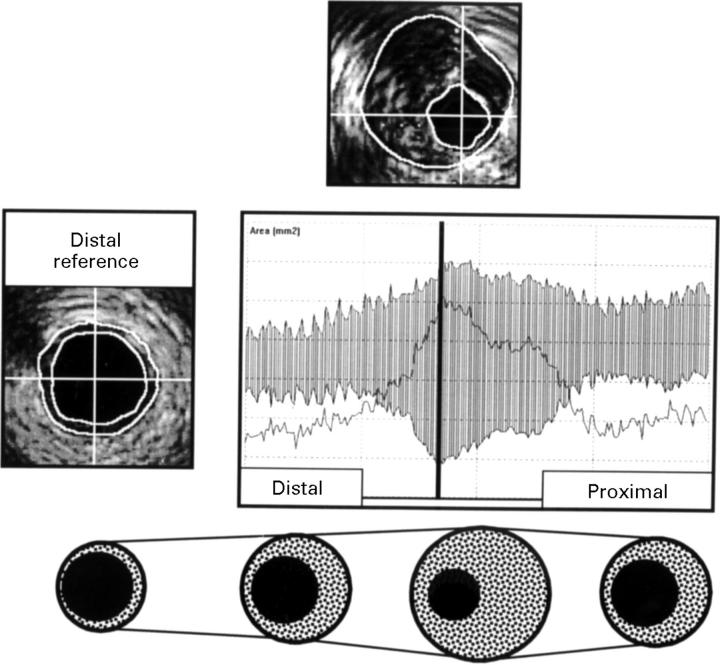
Design: 35 angiographically significant coronary lesions were examined by intravascular ultrasound (IVUS) during motorised transducer pullback. Segments 20 mm in length were analysed using a validated automated three dimensional analysis system. IVUS was used to classify lesions as having inadequate (group I) or adequate (group II) compensatory enlargement.
Results: There was no significant difference in quantitative angiographic measurements and the IVUS minimum lumen cross sectional area between groups I (n = 15) and II (n = 20). In group I, the vessel cross sectional area was 13.3 (3.0) mm2 at the lesion site and 14.4 (3.6) mm2 at the distal reference (p < 0.01), whereas in group II it was 17.5 (5.6) mm2 at the lesion site and 14.0 (6.0) mm2 at the distal reference (p < 0.001). Vessel and plaque cross sectional areas were significantly smaller in group I than in group II (13.3 (3.0) v 17.5 (5.6) mm2, p < 0.01; and 10.9 (2.8) v 15.2 (4.9) mm2; p < 0.005). Similarly, vessel and plaque volume were smaller in group I (291.0 (61.0) v 353.7 (110.0) mm3, and 177.5 (48.4) v 228.0 (92.8) mm3, p < 0.05 for both). Lumen areas and volumes were similar.
Conclusions: In lesions with inadequate compensatory enlargement, both vessel and plaque volume appear to be smaller than in lesions with adequate compensatory enlargement.
Figures


Comment in
-
Coronary artery remodelling.Heart. 1998 Feb;79(2):109-10. doi: 10.1136/hrt.79.2.109. Heart. 1998. PMID: 9538296 Free PMC article. No abstract available.
-
Arterial remodelling and eccentricity of plaque.Heart. 1998 Dec;80(6):633. doi: 10.1136/hrt.80.6.633. Heart. 1998. PMID: 10065040 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical