

Shrinkage of human coronary arteries is an important determinant of de novo atherosclerotic luminal stenosis: an in vivo intravascular ultrasound study
- PMID: 9538306
- PMCID: PMC1728600
- DOI: 10.1136/hrt.79.2.143
Shrinkage of human coronary arteries is an important determinant of de novo atherosclerotic luminal stenosis: an in vivo intravascular ultrasound study
Abstract
Objective: To assess the occurrence of arterial remodelling types and its relation with the severity of luminal stenosis in atherosclerotic coronary arteries.
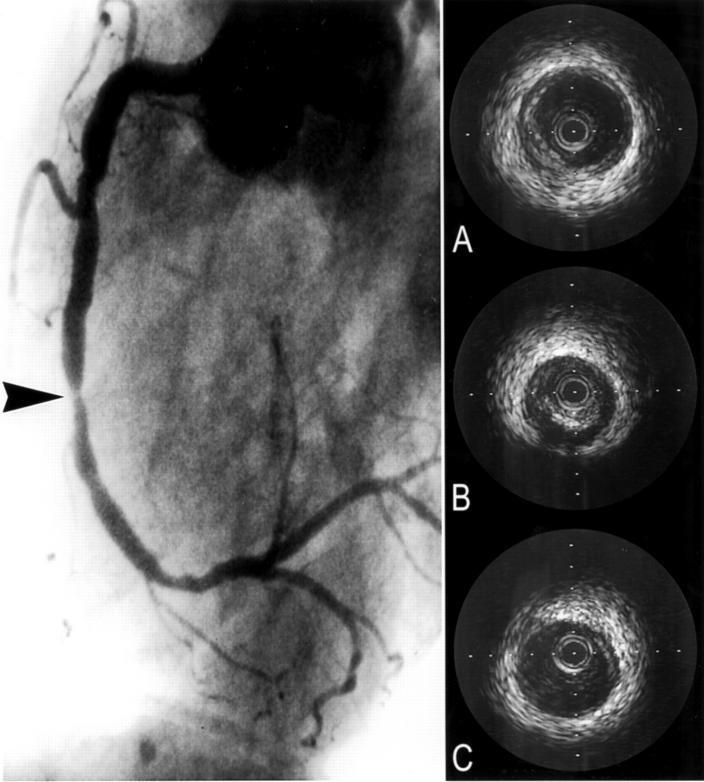
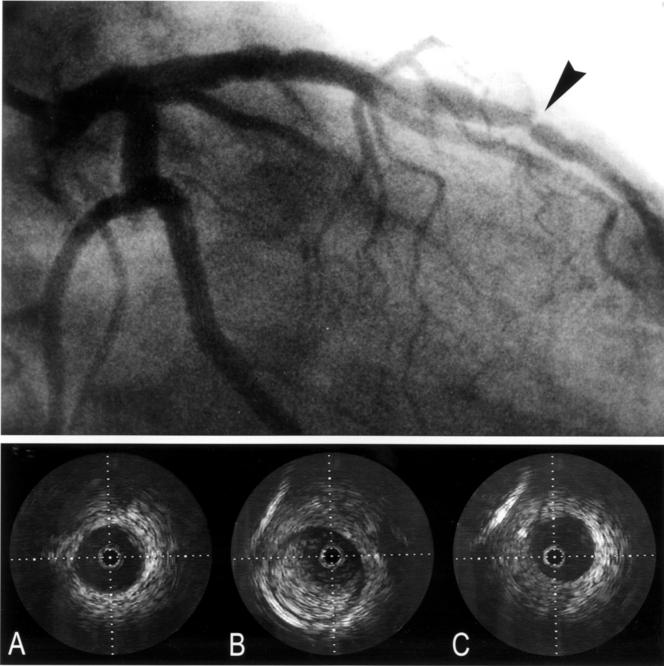
Patients and methods: Twenty one de novo coronary lesions of 20 patients, who were scheduled for percutaneous transluminal coronary angioplasty (PTCA), were investigated with intravascular ultrasound before PTCA. Local arterial remodelling at the lesion site was studied by measuring the cross sectional area circumscribed by the external elastic lamina (EEL) relative to the reference site: (EEL area lesion/reference EEL area) x 100%. Three groups were defined. Group A: relative EEL area of less than 95% (shrinkage), group B: relative EEL area between 95% and 105% (no remodelling), group C: relative increase in EEL area of more than 105% (compensatory enlargement).
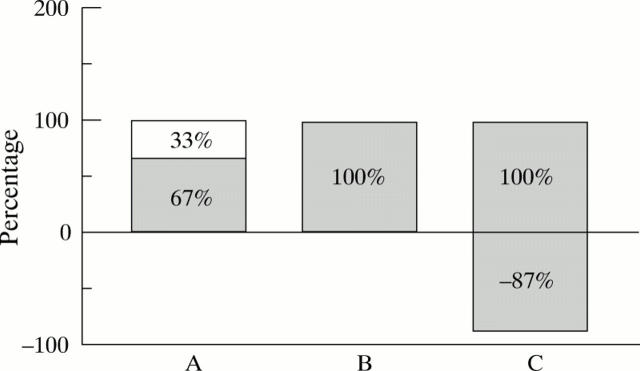
Results: All three types of remodelling were observed at the lesion site: group A (shrinkage) n = 8, group B (no remodelling) n = 5, group C (compensatory enlargement) n = 8. The mean (SD) relative EEL area at the lesion site in group A and C was 83(9)% and 132(30)%, respectively. In group A, 33% of the luminal area stenosis at the lesion site was caused by shrinkage of the artery. In contrast, group C showed that 87% of the plaque area did not contribute to luminal area stenosis because of compensatory arterial enlargement.
Conclusions: These results show that both compensatory enlargement and paradoxical shrinkage occurs in the atherosclerotic coronary artery. Next to plaque accumulation, the type of atherosclerotic remodelling is an important determinant of luminal narrowing.
Figures
Comment in
-
Coronary artery remodelling.Heart. 1998 Feb;79(2):109-10. doi: 10.1136/hrt.79.2.109. Heart. 1998. PMID: 9538296 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical