

Use of immunoblot assay to define serum antibody patterns associated with Helicobacter pylori infection and with H. pylori-related ulcers
- PMID: 9542911
- PMCID: PMC104663
- DOI: 10.1128/JCM.36.4.931-936.1998
Use of immunoblot assay to define serum antibody patterns associated with Helicobacter pylori infection and with H. pylori-related ulcers
Abstract
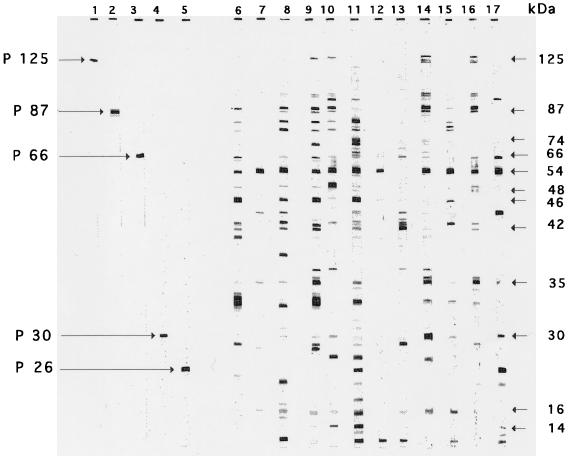
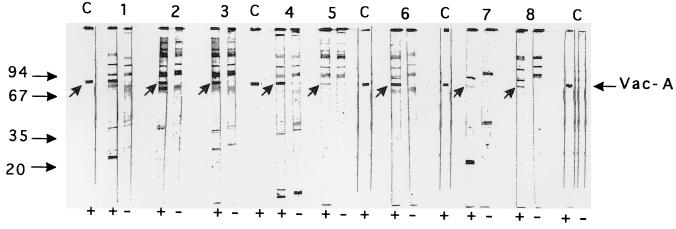
Serology has been used worldwide to detect Helicobacter pylori infection. Using an immunoblot assay with an antigen from strain ATCC 43579, we sought to determine the antibodies which were good markers of colonization and the antibody patterns associated with ulcers or atrophy. Out of 98 dyspeptic patients, 41 were colonized by H. pylori, based on a positive culture or on positive results of both a urease test and direct examination. These 41 patients were seropositive by an enzyme immunoassay, and 12 of them had ulcers and 29 had evidence of atrophy. Fifty-seven of the 98 patients were noncolonized. Twenty-five of the 57 had evidence of gastric atrophy, and 10 were seropositive; 5 of these 10 had ulcers. By Western blot analysis, 12 antibodies were significantly more frequent in sera from colonized patients, and they produced immunoreactive bands at 125, 87, 74, 66, 54, 48, 46, 42, 35, 30, 16 and 14 kDa. The presence of at least one band at 54, 35, or 42 kDa was the best marker of infection (sensitivity, 95%; specificity, 82%). In the group of colonized patients, none of the antibody patterns were correlated to gastric atrophy. Conversely, the presence of a band at 125, 87, or 35 kDa was statistically associated with the presence of an ulcer. The simultaneous presence of bands at 87 and 35 kDa predicted the risk of ulcers with 83% sensitivity and 69% specificity. By using CagA-positive and VacA-positive strains and CagA-negative and VacA-negative isogenic mutants, the antigens corresponding to the bands at 125 and 87 kDa were shown to be CagA and VacA, respectively. On the other hand, the 35-kDa antigen is a novel uncharacterized component of H. pylori. These results may help to optimize the composition of antigenic preparations for serologic detection of H. pylori colonization. Immunoblot assay would be useful for screening patients at high risk of ulcers.
Figures
References
-
- Andersen L P. The antibody response to Helicobacter pylori infection, and the value of serologic tests to detect H. pylori and for post-treatment monitoring. In: Goodwin C S, Worsley B W, editors. Helicobacter pylori: biology and clinical practice. Boca Raton, Fla: CRC Press; 1993. pp. 285–306.
-
- Blaser M J, Perez-Perez G, Kleanthous H, Cover T L, Peek R M, Chyou P H, Stemmermann G N, Nomura A. Infection with Helicobacter pylori strains possessing cagA is associated with increased risk of developing adenocarcinoma of the stomach. Cancer Res. 1995;55:2111–2115. - PubMed
-
- Calam J. The pathogenesis of Helicobacter pylori infection and duodenal ulcer: the role of gastrin and other soluble factors. In: Goodwin C S, Worsley B W, editors. Helicobacter pylori: biology and clinical practice. Boca Raton, Fla: CRC Press; 1993. pp. 239–256.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
