

Review
doi: 10.1136/bmj.316.7138.1140.
The role of nuclear medicine in clinical investigation
Affiliations
- PMID: 9552956
- PMCID: PMC1112941
- DOI: 10.1136/bmj.316.7138.1140
Item in Clipboard
Review
The role of nuclear medicine in clinical investigation
BMJ.
.
No abstract available
Figures
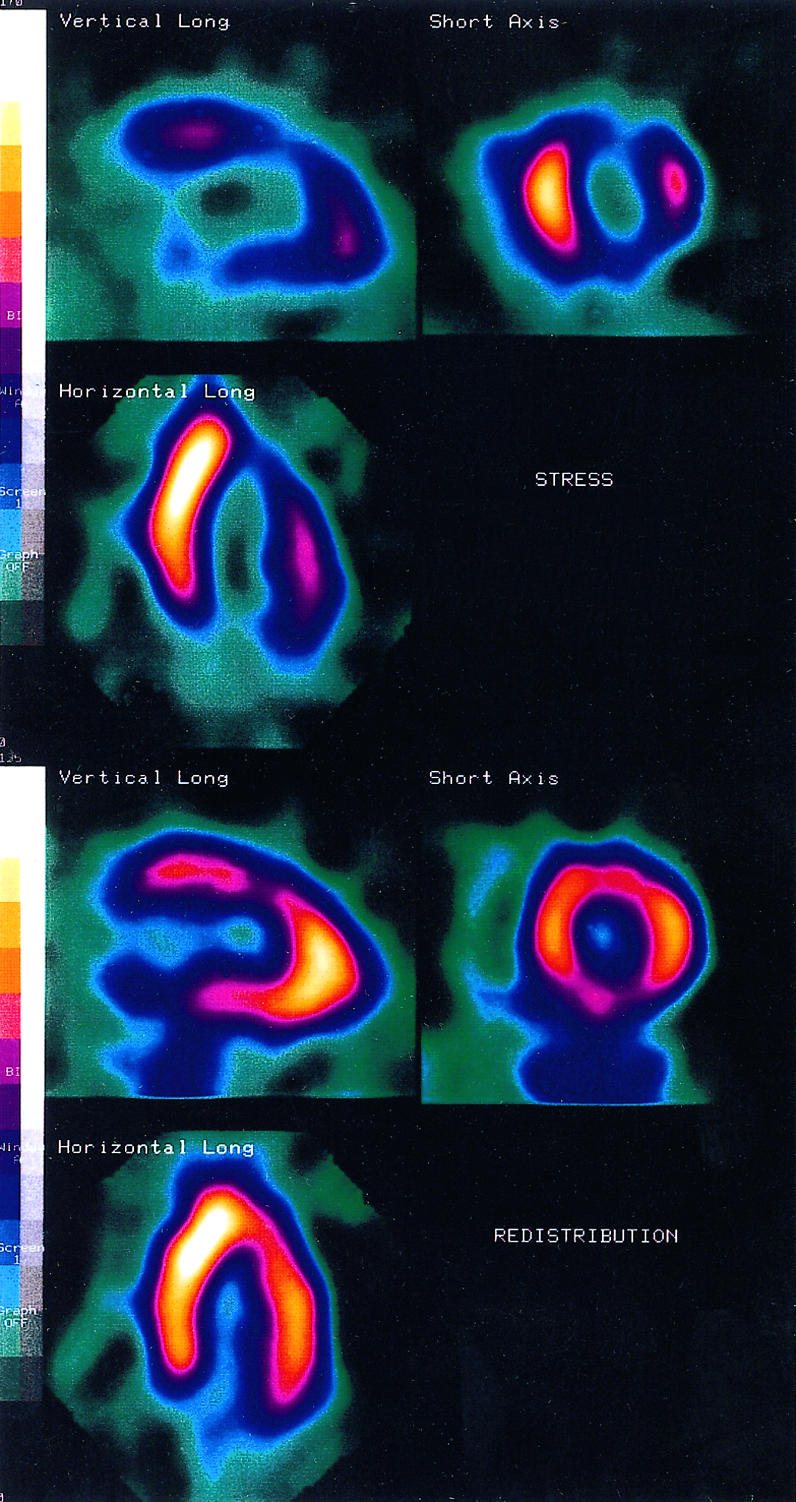
201Tl myocardial perfusion images in a patient with exertional chest pain. Reversible ischaemia of the anterior, inferior, and lateral walls suggests a high probability of future cardiac events
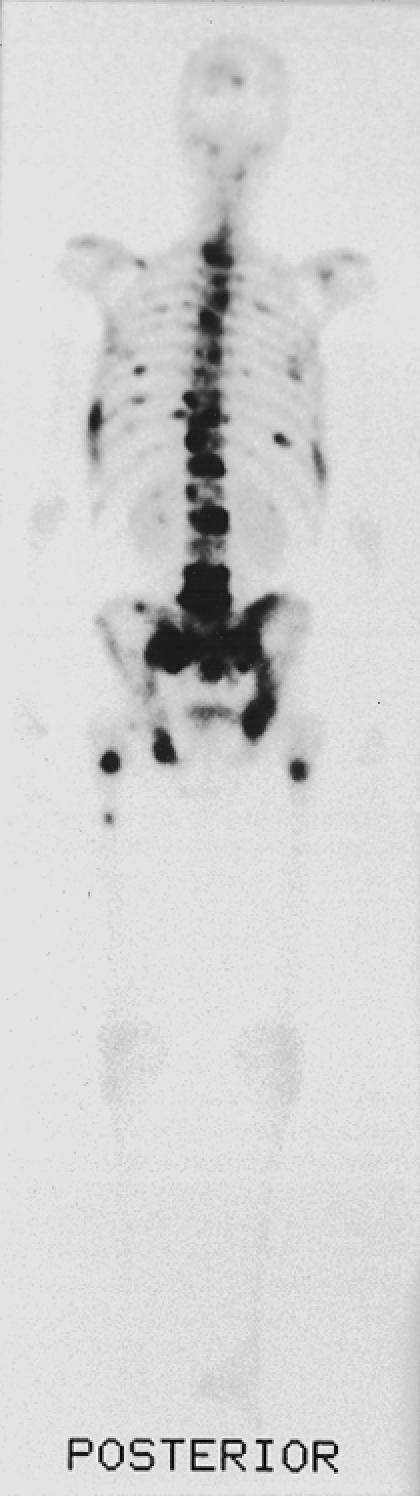
99mTc-MDP bone scan in a patient with carcinoma of the prostate and pelvic pain. Multiple focal areas of increased tracer activity throughout the skeleton (including the pelvis, spine, ribs, skull, and femurs) indicate widespread bony metastases
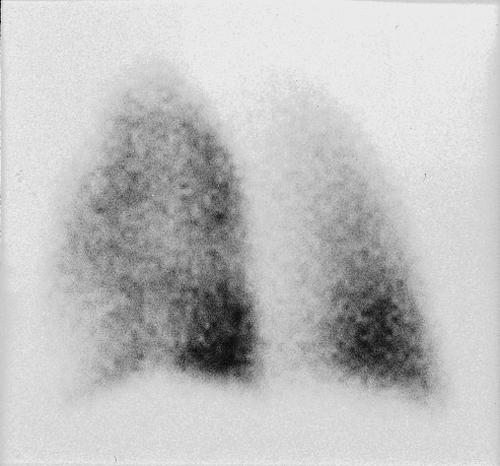
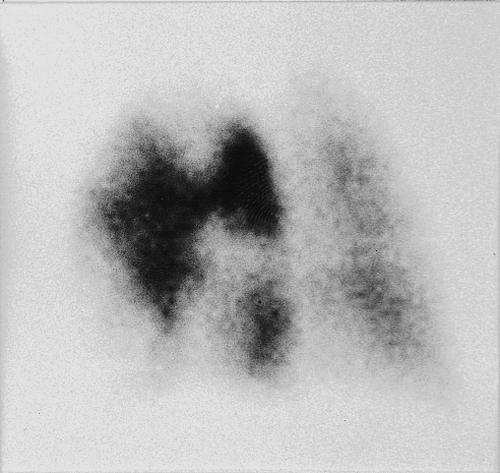
Ventilation-perfusion lung scan (left posterior oblique views: (left) ventilation; (right) perfusion) in a patient with dyspnoea and pleuritic chest pain. There are multiple perfusion defects which are ventilated. High probability of pulmonary embolism
Ventilation-perfusion lung scan (left posterior oblique views: (left) ventilation; (right) perfusion) in a patient with dyspnoea and pleuritic chest pain. There are multiple perfusion defects which are ventilated. High probability of pulmonary embolism
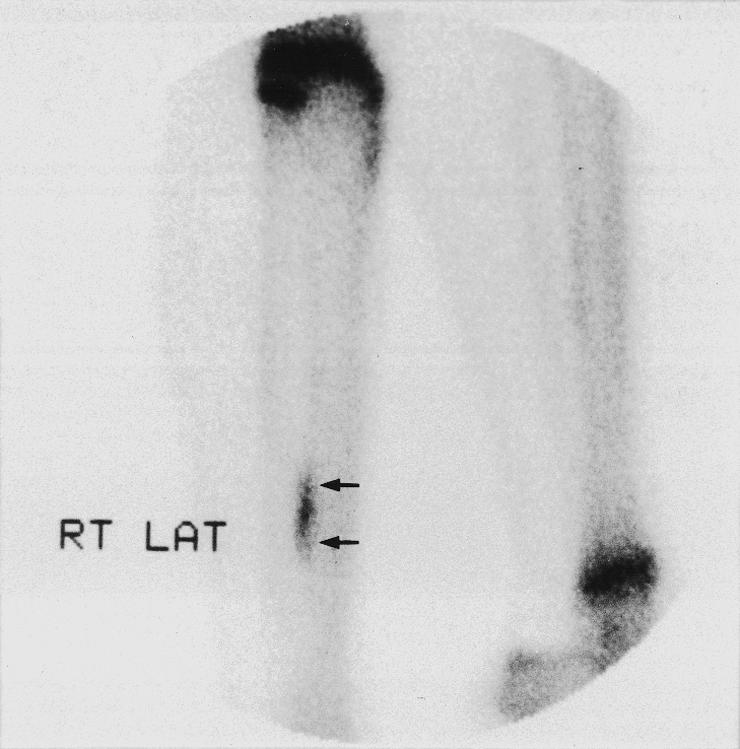
99mTc-MDP bone scan of painful legs in athlete. Elongated focus of increased activity along posterior third of tibial shaft is typical of shin splint
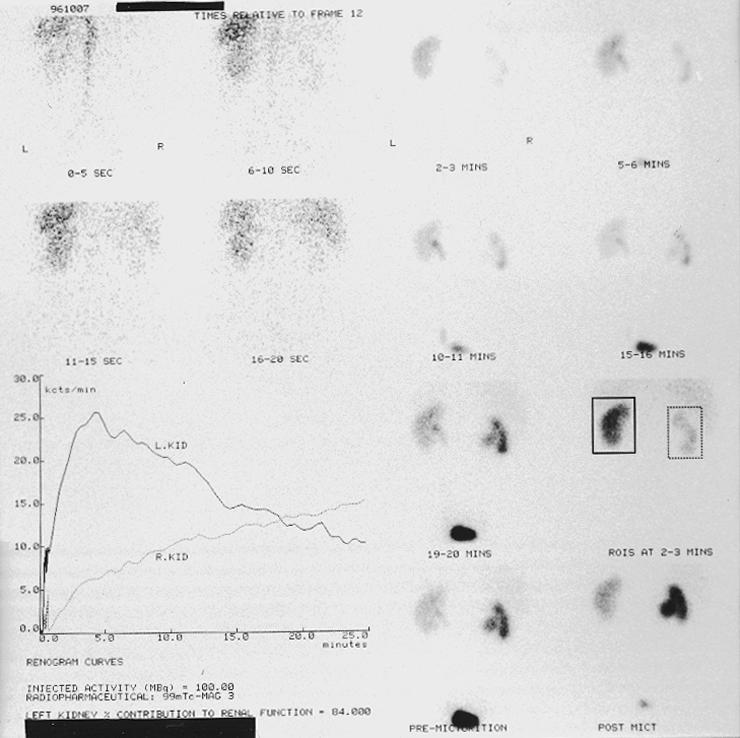
99mTc-MAG3 renogram in patient with stent inserted for right pelvi-ureteric obstruction. Right kidney shows sluggish tracer excretion. No significant drainage even after 40 mg frusemide was given, compatible with right obstructive uropathy
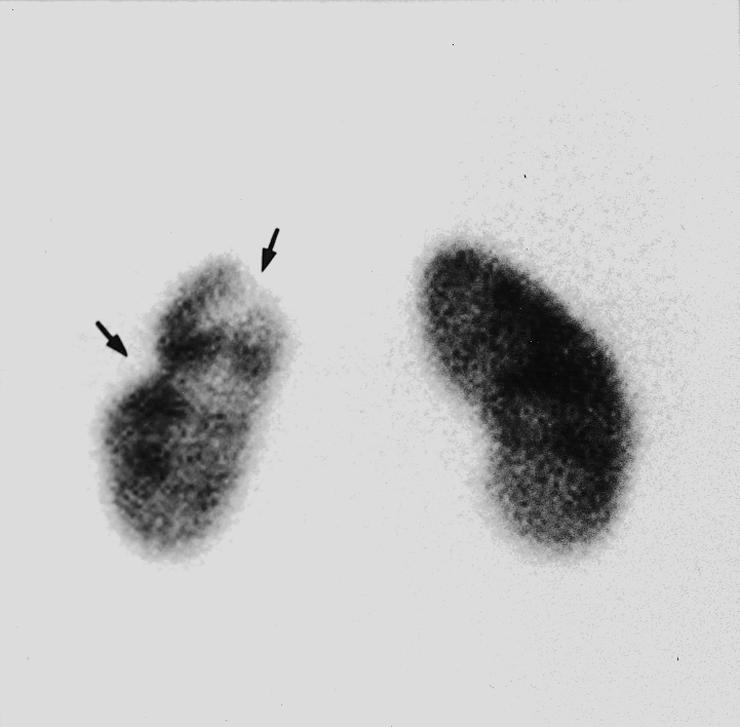
99mTc-DMSA scan (posterior view) in patient with recurrent urinary tract infection. Cortical defects (arrows) at upper pole and lateral margin of left kidney indicate scarring

111In white cell study (anterior view) in patient with newly diagnosed Crohn’s disease. Increased tracer activity in ileocaecal region and entire colon indicates diffuse active inflammatory bowel disease
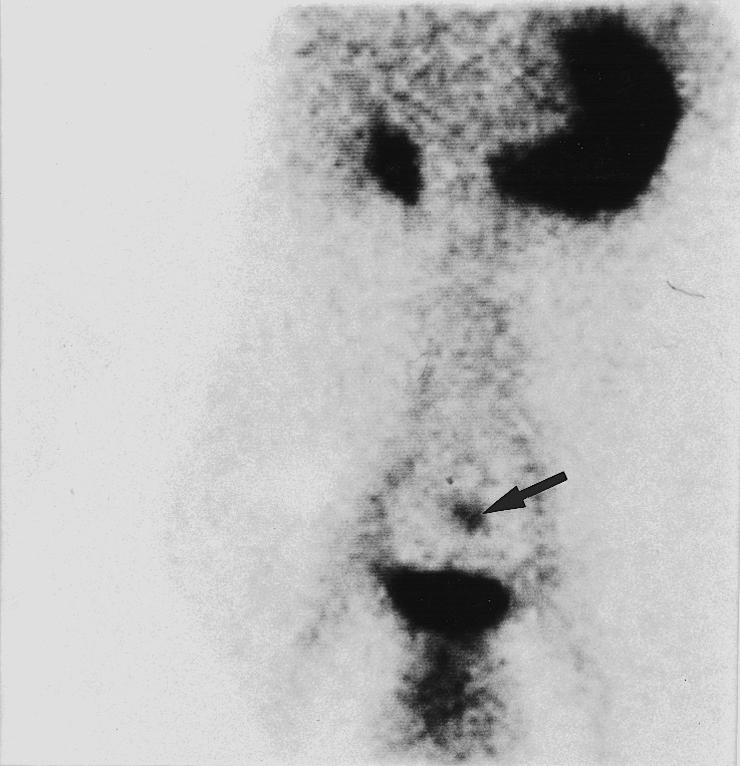
99mTc-pertechnetate Meckel’s scan (anterior view) in patient with gastrointestinal bleeding. Increased tracer activity within Meckel’s diverticulum (arrow); normal tracer uptake in stomach and adjacent right renal pelvis
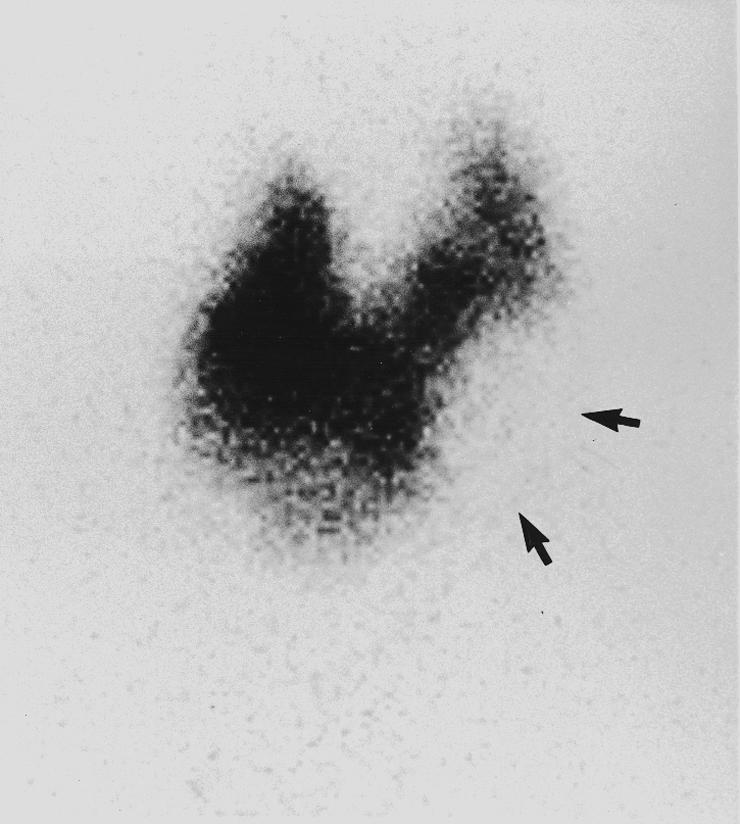
123I scan in patient with thyroid swelling. Irregular tracer uptake in enlarged multinodular thyroid gland; dominant “cold” area in left thyroid lobe (arrow). Subsequent biopsy showed colloid cyst
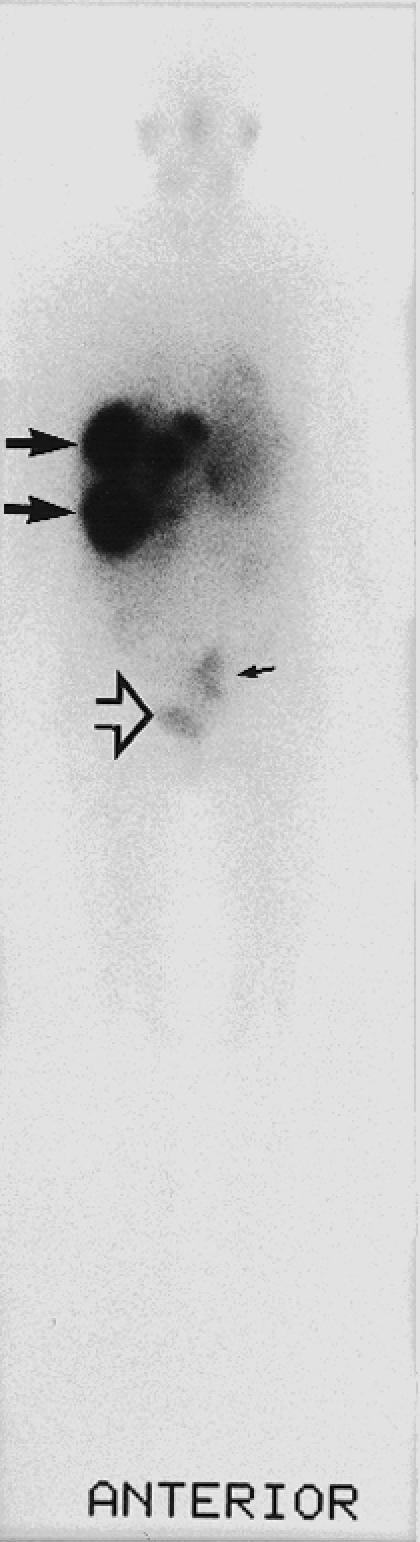
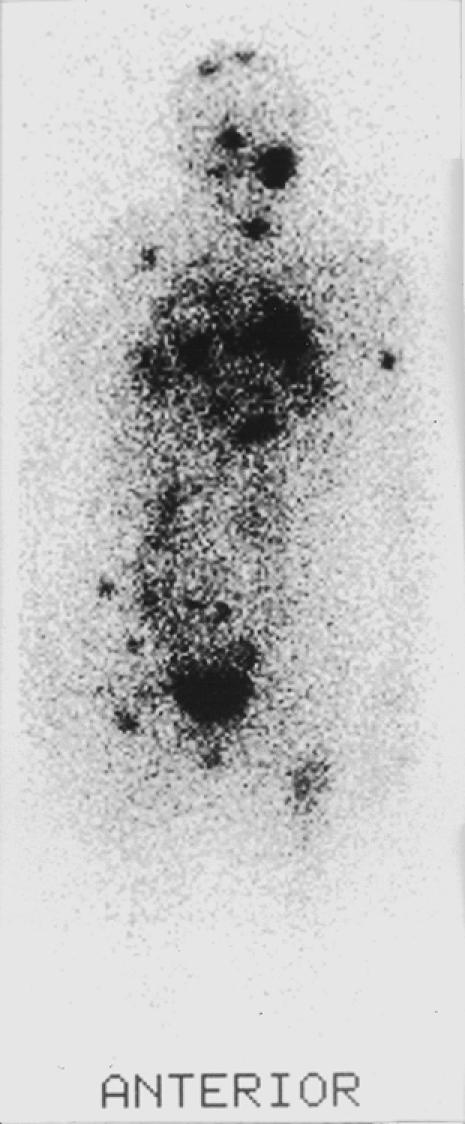
(left) 123I-MIBG scan in patient with malignant carcinoid and liver metastases to assess suitability for treatment with 131I-MIBG. Several areas of intense tracer uptake in liver, particularly within right lobe (two medium arrows) and pelvis (small arrow) to left of bladder (open arrow). 123I-MIBG avid carcinoid metastases suitable for 131I-MIBG therapy Fig 11 (right) 131I follow up scan in patient with differentiated carcinoma of thyroid. Multiple focal areas of increased tracer uptake (including skull, left cervical nodes, lungs, lower abdomen, femurs). 131I avid carcinoma thyroid metastases suitable for radioiodine therapy
(left) 123I-MIBG scan in patient with malignant carcinoid and liver metastases to assess suitability for treatment with 131I-MIBG. Several areas of intense tracer uptake in liver, particularly within right lobe (two medium arrows) and pelvis (small arrow) to left of bladder (open arrow). 123I-MIBG avid carcinoid metastases suitable for 131I-MIBG therapy Fig 11 (right) 131I follow up scan in patient with differentiated carcinoma of thyroid. Multiple focal areas of increased tracer uptake (including skull, left cervical nodes, lungs, lower abdomen, femurs). 131I avid carcinoma thyroid metastases suitable for radioiodine therapy
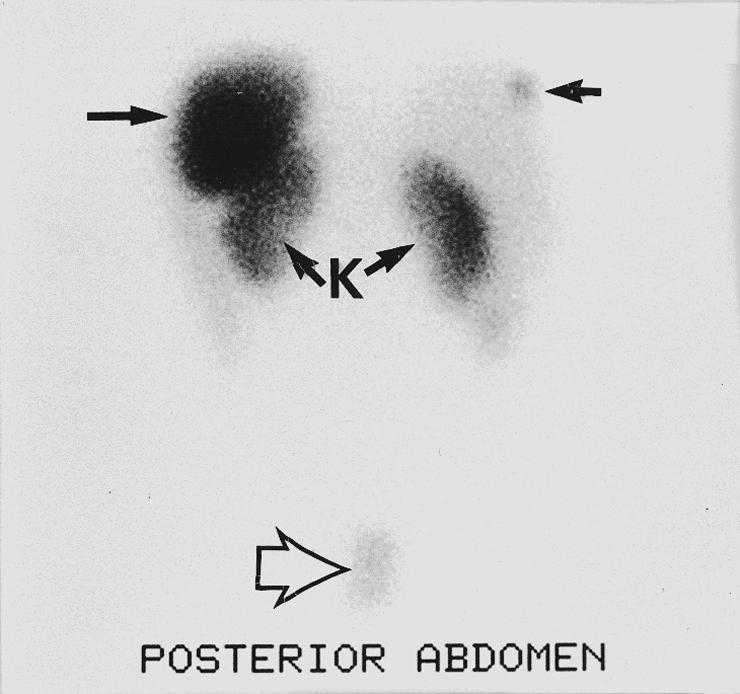
111In-pentetreotide scan in patient with malignant carcinoid and liver metastases proved by biopsy not seen on abdominal spiral computed tomography scan. Normal distribution of 111In-pentetreotide to spleen (large arrow) and kidneys (K); small focal area of increased tracer activity in right lobe of liver (small arrow on right), indicating lesion positive for somatostatin receptor
References
-
- Pennell DJ, Prvulovich EM. Clinician’s guide to nuclear medicine: nuclear cardiology. Hatfield: Impact Healthcare; 1995.
-
- McKillop JH, Fogelman I. Clinician’s guide to nuclear medicine: benign and malignant bone disease. London: Churchill Livingstone; 1991.
-
- Testa HJ, Prescott MC. Clinician’s guide to nuclear medicine: nephrourology. Hatfield: Impact Healthcare; 1996.
-
- Harding LK, Robinson PJA. Clinician’s guide to nuclear medicine: gastroenterology. London: Churchill Livingstone; 1990.
-
- Costa DC, Ell PJ. Clinician’s guide to nuclear medicine: blood flow in neurology and psychiatry. London: Churchill Livingstone; 1991.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources