

Incidence and severity of acute allograft rejection in liver transplant recipients treated with alfa interferon
- PMID: 9563957
- PMCID: PMC3005707
- DOI: 10.1002/lt.500040315
Incidence and severity of acute allograft rejection in liver transplant recipients treated with alfa interferon
Abstract
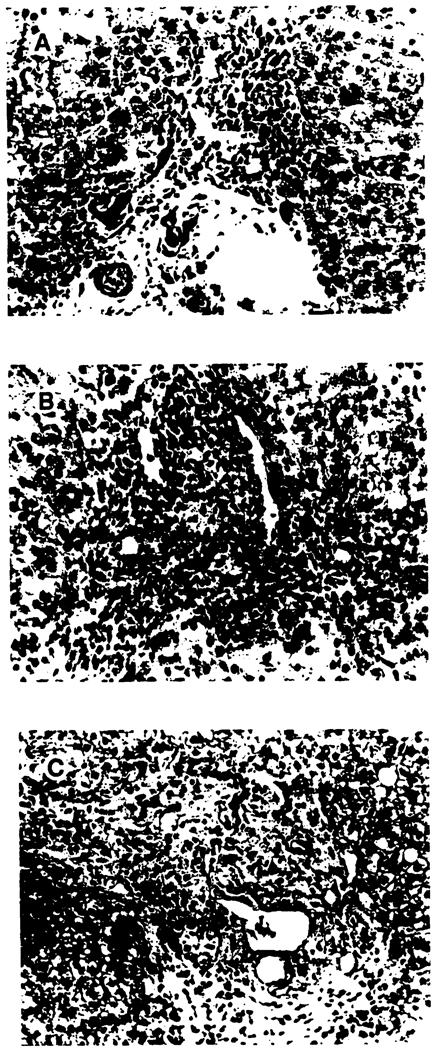
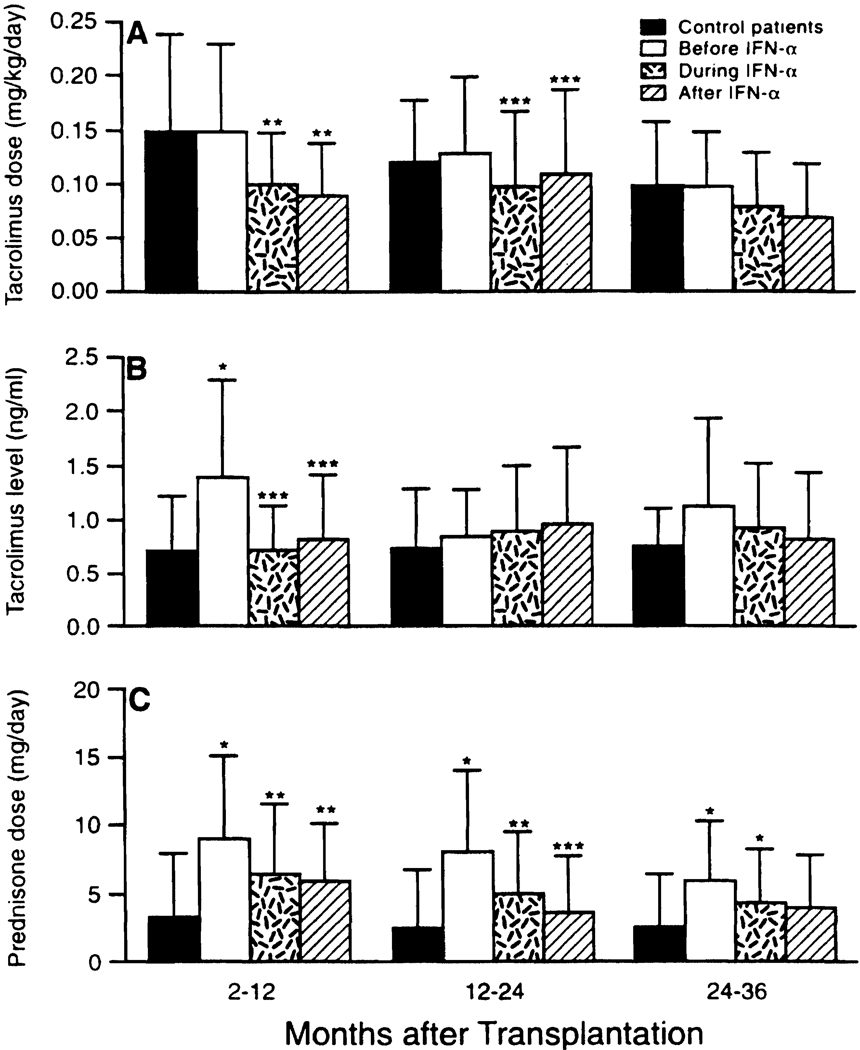
Interferon alfa-2b (IFN-alpha) therapy has been shown to be effective in the treatment of viral hepatitis B (HBV) or viral hepatitis C (HCV) in patients who did not undergo transplantation. However, in allograft recipients, treatment with IFN-alpha often leads to allograft rejection. The aim of the present study was to determine if IFN-alpha therapy increases the incidence or severity of acute rejection in human liver allograft recipients. One hundred five orthotopic liver transplant (OLT) recipients with HBV (n = 32), HCV (n = 58), or Non A Non B Non C (n = 15) viral infections were treated with a 6-month course of IFN-alpha, 5 million U subcutaneously three times a week, which began 2 to 97 months after transplantation. The mean hepatitis activity index (HAI) at the beginning of the therapy was 10.1 +/- 3.0. The baseline immunosuppression was achieved by tacrolimus in 77 patients and by cyclosporine A (CyA) in 28 patients. Contemporaneous controls consisted of 132 OLT patients (100 who received tacrolimus and 32 who received CyA) who did not receive IFN-alpha. A retrospective analysis was performed on this group of patients. The incidence of rejection and the baseline immunosuppression were compared. All biopsies were reviewed without knowledge of clinical data and scored for HAI and for rejection activity index (RAI). The biochemical response to IFN-alpha was also examined. The mean baseline maintenance dose of prednisone was greater by 2 mg daily in patients who received IFN-alpha with tacrolimus compared with control patients who did not receive IFN-alpha with tacrolimus (IFN-alpha 5. 3 +/- 5.2 mg daily v controls 3.3 +/- 4.9 mg daily; P </= .05). Similarly, the mean maintenance dose of prednisone was greater by 2.5 mg daily in patients who received IFN-alpha compared with controls who received CyA-based immunosuppression (IFN-alpha 9.8 +/- 3.1 mg daily v controls 7.3 +/- 3.3 mg daily; P = .01). Acute rejection episodes were detected in 10.5% (n = 11) of IFN-alpha-treated patients compared with 8.8% of controls for the similar time period from OLT and period of exposure to risk of rejection. Mean RAI was 2.0 +/- 2.4 for the IFN-alpha-treated group and 2.1 +/- 1.7 for controls. Rejection episodes with IFN-alpha treatment were mild and responded to steroid therapy. In OLT recipients, the risk of acute rejection was not increased by the introduction of IFN-alpha. However, in this study, patients were exposed to greater levels of immunosuppression.
Copyright 1998 W.B. Saunders Company.
Figures
Similar articles
-
Successful treatment of fibrosing cholestatic hepatitis after liver transplantation.Transplant Proc. 2011 Apr;43(3):905-8. doi: 10.1016/j.transproceed.2011.02.034. Transplant Proc. 2011. PMID: 21486625
-
Anti-IL2 induction in liver transplantation with 93% rejection-free patient and graft survival at 18 months.J Surg Res. 2007 Apr;138(2):198-204. doi: 10.1016/j.jss.2006.08.025. Epub 2007 Feb 8. J Surg Res. 2007. PMID: 17292404
-
Effects of interferon treatment on liver histology and allograft rejection in patients with recurrent hepatitis C following liver transplantation.Liver Transpl. 2004 Jul;10(7):850-8. doi: 10.1002/lt.20189. Liver Transpl. 2004. PMID: 15237368
-
The effects of HLA mismatching and immunosuppressive therapy on early rejection outcome in pediatric heart transplant recipients.J Heart Lung Transplant. 1998 Dec;17(12):1195-200. J Heart Lung Transplant. 1998. PMID: 9883760
-
The clinical and immunologic impact of using interferon and ribavirin in the immunosuppressed host.Liver Transpl. 2003 Nov;9(11):S79-89. doi: 10.1053/jlts.2003.50257. Liver Transpl. 2003. PMID: 14586901 Review.
Cited by
-
Immunosuppression for liver transplantation in HCV-infected patients: mechanism-based principles.Liver Transpl. 2005 Nov;11(11):1343-52. doi: 10.1002/lt.20536. Liver Transpl. 2005. PMID: 16237712 Free PMC article.
-
Is there increased risk of hepatocellular carcinoma recurrence in liver transplant patients with direct-acting antiviral therapy?Hepatol Int. 2019 Mar;13(2):190-198. doi: 10.1007/s12072-019-09930-x. Epub 2019 Jan 24. Hepatol Int. 2019. PMID: 30680672
-
Hepatic and intestinal transplantation at the University of Pittsburgh.Clin Transpl. 1998:263-86. Clin Transpl. 1998. PMID: 10503105 Free PMC article. No abstract available.
References
-
- Ferrell LD, Wright TL, Roberts J, Acher N, Lake J. Hepatitis C viral infection in liver transplant recipients. Hepatology. 1992;16:865–876. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
