

Clinical, cellular, and molecular factors that contribute to antifungal drug resistance
- PMID: 9564569
- PMCID: PMC106838
- DOI: 10.1128/CMR.11.2.382
Clinical, cellular, and molecular factors that contribute to antifungal drug resistance
Abstract
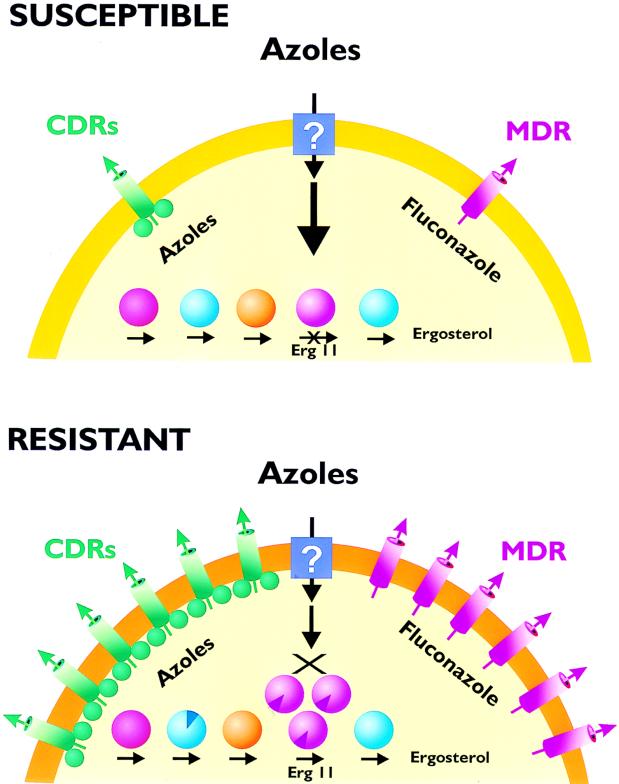
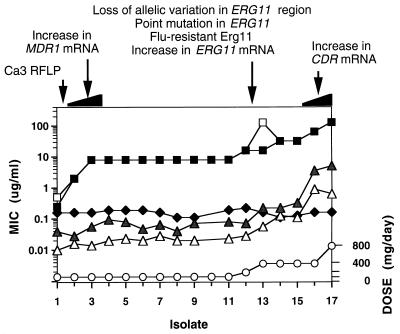
In the past decade, the frequency of diagnosed fungal infections has risen sharply due to several factors, including the increase in the number of immunosuppressed patients resulting from the AIDS epidemic and treatments during and after organ and bone marrow transplants. Linked with the increase in fungal infections is a recent increase in the frequency with which these infections are recalcitrant to standard antifungal therapy. This review summarizes the factors that contribute to antifungal drug resistance on three levels: (i) clinical factors that result in the inability to successfully treat refractory disease; (ii) cellular factors associated with a resistant fungal strain; and (iii) molecular factors that are ultimately responsible for the resistance phenotype in the cell. Many of the clinical factors that contribute to resistance are associated with the immune status of the patient, with the pharmacology of the drugs, or with the degree or type of fungal infection present. At a cellular level, antifungal drug resistance can be the result of replacement of a susceptible strain with a more resistant strain or species or the alteration of an endogenous strain (by mutation or gene expression) to a resistant phenotype. The molecular mechanisms of resistance that have been identified to date in Candida albicans include overexpression of two types of efflux pumps, overexpression or mutation of the target enzyme, and alteration of other enzymes in the same biosynthetic pathway as the target enzyme. Since the study of antifungal drug resistance is relatively new, other factors that may also contribute to resistance are discussed.
Figures
References
-
- Alarco A M, Balan I, Talibi D, Mainville N, Raymond M. AP1-mediated multidrug resistance in Saccharomyces cerevisiae requires FLR1 encoding a transporter of the major facilitator superfamily. J Biol Chem. 1997;272:19304–19313. - PubMed
-
- Alexander B D, Perfect J R. Antifungal resistance trends towards the year 2000: Implications for therapy and new approaches. Drugs. 1997;54:657–678. - PubMed
-
- Arthington B A, Bennett L G, Skatrud P L, Guynn C J, Barbuch R J, Ulbright C E, Bard M. Cloning, disruption and sequence of the gene encoding yeast C-5 sterol desaturase. Gene. 1991;102:39–44. - PubMed
-
- Baily G G, Moore C B, Essayag S M, deWit S, Burnie J P, Denning D W. Candida inconspicua, a fluconazole-resistant pathogen in patients infected with human immunodeficiency virus. Clin Infect Dis. 1997;25:161–163. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
