

Systematic review of efficacy of cognitive behaviour therapies in childhood and adolescent depressive disorder
- PMID: 9596592
- PMCID: PMC28555
- DOI: 10.1136/bmj.316.7144.1559
Systematic review of efficacy of cognitive behaviour therapies in childhood and adolescent depressive disorder
Abstract
Objective: To determine whether cognitive behaviour therapy is an effective treatment for childhood and adolescent depressive disorder.
Design: Systematic review of six randomised trials comparing the efficacy of cognitive behaviour therapy with inactive interventions in subjects aged 8 to 19 years with depressive disorder.
Main outcome measure: Remission from depressive disorder.
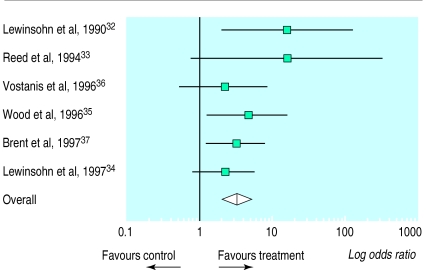
Results: The rate of remission from depressive disorder was higher in the therapy group (129/208; 62%) than in the comparison group (61/168; 36%). The pooled odds ratio was 3.2 (95% confidence interval 1.9 to 5.2), suggesting a significant benefit of active treatment. Most studies, however, were based on relatively mild cases of depression and were of only moderate quality.
Conclusions: Cognitive behaviour therapy may be of benefit for depressive disorder of moderate severity in children and adolescents. It cannot, however, yet be recommended for severe depression. Definitive large trials will be required to determine whether the results of this systematic review are reliable.
Figures
Comment in
-
Depression in children.BMJ. 2002 Aug 3;325(7358):229-30. doi: 10.1136/bmj.325.7358.229. BMJ. 2002. PMID: 12153903 Free PMC article. No abstract available.
Similar articles
-
Low-Intensity Guided Help Through Mindfulness (LIGHTMIND): study protocol for a randomised controlled trial comparing supported mindfulness-based cognitive therapy self-help to supported cognitive behavioural therapy self-help for adults experiencing depression.Trials. 2020 May 4;21(1):374. doi: 10.1186/s13063-020-04322-1. Trials. 2020. PMID: 32366320 Free PMC article.
-
Nonsomatic treatment of depression.Child Adolesc Psychiatr Clin N Am. 2002 Jul;11(3):579-93. doi: 10.1016/s1056-4993(02)00009-3. Child Adolesc Psychiatr Clin N Am. 2002. PMID: 12222084 Review.
-
Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care with and without cognitive behaviour therapy in adolescents with major depression: randomised controlled trial.BMJ. 2007 Jul 21;335(7611):142. doi: 10.1136/bmj.39224.494340.55. Epub 2007 Jun 7. BMJ. 2007. PMID: 17556431 Free PMC article. Clinical Trial.
-
Internet-based psychodynamic versus cognitive behaviour therapy for adolescents with depression: study protocol for a non-inferiority randomized controlled trial (the ERiCA study).Trials. 2020 Jun 29;21(1):587. doi: 10.1186/s13063-020-04491-z. Trials. 2020. PMID: 32600400 Free PMC article.
-
Psychological therapies for the treatment of post-traumatic stress disorder in children and adolescents (Review).Evid Based Child Health. 2013 May;8(3):1004-116. doi: 10.1002/ebch.1916. Evid Based Child Health. 2013. PMID: 23877914 Review.
Cited by
-
The effects of cognitive-behavioural therapy on mood-related ruminative response style in depressed adolescents.Child Adolesc Psychiatry Ment Health. 2008 Jan 29;2(1):3. doi: 10.1186/1753-2000-2-3. Child Adolesc Psychiatry Ment Health. 2008. PMID: 18230146 Free PMC article.
-
Treading a fine line: is diagnosing depression in young people just medicalising moodiness?Br J Gen Pract. 2009 Mar;59(560):156-7. doi: 10.3399/bjgp09X407081. Br J Gen Pract. 2009. PMID: 19275830 Free PMC article. No abstract available.
-
Screening and early psychological intervention for depression in schools : systematic review and meta-analysis.Eur Child Adolesc Psychiatry. 2006 Aug;15(5):300-7. doi: 10.1007/s00787-006-0537-4. Epub 2006 Mar 29. Eur Child Adolesc Psychiatry. 2006. PMID: 16572276
-
Clinical review of mania, hostility and suicide-related events in children and adolescents treated with antidepressants.Paediatr Child Health. 2005 Oct;10(8):457-63. Paediatr Child Health. 2005. PMID: 19668657 Free PMC article.
-
Major depressive disorder in children and adolescents.Ment Health Clin. 2018 Nov 1;8(6):275-283. doi: 10.9740/mhc.2018.11.275. eCollection 2018 Nov. Ment Health Clin. 2018. PMID: 30397569 Free PMC article.
References
-
- Kolvin I, Barrett ML, Bhate SR, Berney TP, Famuyiwa OO, Fundudis T, et al. The Newcastle child depression project: diagnosis and classification of depression. Br J Psychiatry. 1991;159 (suppl 11):9–21. - PubMed
-
- Harrington RC. Affective disorders. In: Rutter M, Taylor E, Hersov L, editors. Child and adolescent psychiatry: modern approaches. 3rd ed. Oxford: Blackwell Scientific; 1994. pp. 330–350.
-
- Emslie G, Rush A, Weinberg W, Kowatch R, Hughes C, Carmody T, et al. A double-blind, randomized placebo-controlled trial of fluoxetine in depressed children and adolescents. Arch Gen Psychiatry. 1997;54:1031–1037. - PubMed
-
- Simeon JG, Dinicola VF, Ferguson HB, Copping W. Adolescent depression: a placebo-controlled fluoxetine treatment study and follow-up. Prog Neuro-Psychopharm Biol Psychiatry. 1990;14:791–795. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources