

Case Reports
doi: 10.1136/hrt.79.4.417.
Prevention of torsade de pointes in the congenital long QT syndrome: use of a pause prevention pacing algorithm
Affiliations
- PMID: 9616356
- PMCID: PMC1728655
- DOI: 10.1136/hrt.79.4.417
Item in Clipboard
Case Reports
Prevention of torsade de pointes in the congenital long QT syndrome: use of a pause prevention pacing algorithm
Heart.
1998 Apr.
Abstract
Torsade de pointes in the congenital long QT syndrome (LQTS) is often pause dependent. Thus, the main goal of pacemaker treatment in the LQTS may be the prevention of pauses that facilitate the onset of torsade de pointes. A pause prevention pacing algorithm (rate smoothing) was used for arrhythmia prevention in a 14 year old girl with congenital LQTS. By temporarily increasing the pacing rate after spontaneous premature beats, rate smoothing down of 18% prevented postextrasystolic pauses, pause related T-U changes, and recurrence of pause induced torsade de pointes. Rate smoothing is a potentially useful tool that ought to be evaluated for the prevention of torsade de pointes in the LQTS.
Figures
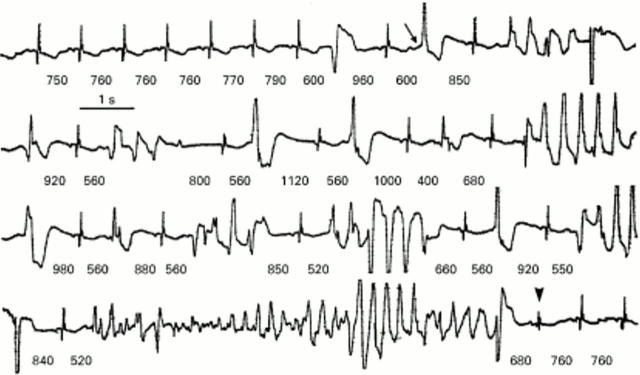
Representative example of pause dependent torsade de pointes. The R-R intervals (shown in milliseconds) gradually increase due to sinus arrhythmia until a sinus cycle of 790 ms is followed by the first premature depolarisation. This extrasystole generates a longer pause (a postextrasystolic pause of 960 ms), which is followed by a sinus complex with postextrasystolic U wave augmentation (arrow) and a new premature depolarisation. The long-short sequence is perpetuated, leading to longer and faster runs of torsade de pointes. Fortuitously, the longest run is followed by a relatively short sinus cycle (arrowhead) and the vicious cycle (long-short sequence) terminates.
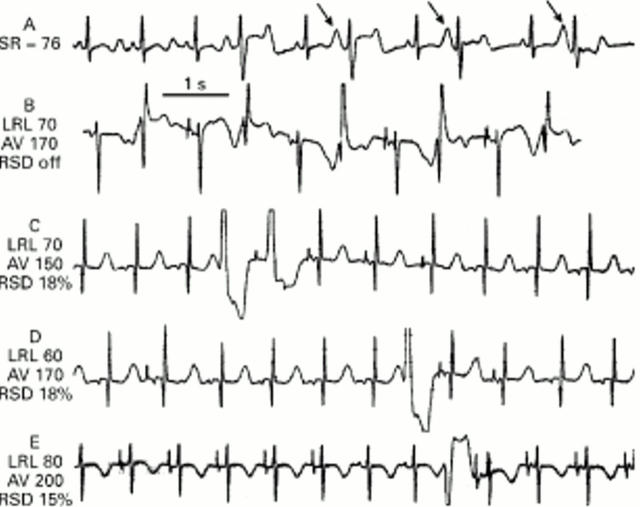
Electrocardiograms following implantation of a permanent DDDR pacemaker with rate smoothing algorithm. SR, sinus rate; LRL, AV, and RSD, programmed lower rate limit (beats/min), AV delay (in milliseconds), and rate smoothing down values (expressed as percentage of the previous R-R interval), respectively. (A) Sinus rate 76 beats/min; a premature complex is followed by a postextrasystolic pause. The ensuing sinus complex has marked post-pause U wave changes (arrow). Ventricular bigeminy (long-short sequence) supervenes. (B) DDD pacing (atrial capture with atrioventricular conduction). Rate smoothing is off. Spontaneous extrasystoles are sensed appropriately, resetting the pacemaker and causing short-long sequences that are perpetuated as ventricular bigeminy. Note the marked postextrasystolic T-U changes after each long interval. (C) Rate smoothing down of 18% during pacing with a relatively slow lower rate limit. After three sinus complexes there is a spontaneous extrasystole. Due to rate smoothing, DDD pacing occurs at a rate faster than the programmed lower rate limit: the first paced cycle is 18% longer than the coupling interval of the extrasystole. There is no atrial capture and there is retrograde conduction from the paced ventricular complex. The next three complexes show atrial pacing and capture with normal atrioventricular conduction. Each paced cycle is 18% longer than the previous one until sinus rhythm ensues. Note the absence of pauses and the absence of T-U changes. (D) Another example of rate smoothing down during DDD pacing with a slow lower rate limit (60 beats/min). An extrasystole triggers atrial pacing (with atrioventricular conduction) and the rate decreases by 18% each cycle. (E) Pacing at 80 beats/min and rate smoothing down of 15%. An extrasystole is followed by more rapid pacing. The first paced complex shows atrial capture and ventricular pseudofusion.
Similar articles
-
Arrhythmias in the congenital long QT syndrome: how often is torsade de pointes pause dependent?Heart. 2000 Jun;83(6):661-6. doi: 10.1136/heart.83.6.661. Heart. 2000. PMID: 10814624 Free PMC article. Review.
-
Rate smoothing with cardiac pacing for preventing torsade de pointes.Am J Cardiol. 2000 Nov 2;86(9A):111K-115K. doi: 10.1016/s0002-9149(00)01228-5. Am J Cardiol. 2000. PMID: 11084109 Review.
-
Mode of onset of torsade de pointes in congenital long QT syndrome.J Am Coll Cardiol. 1996 Nov 1;28(5):1262-8. doi: 10.1016/s0735-1097(96)00311-7. J Am Coll Cardiol. 1996. PMID: 8890825
-
Cardiac pacing in the long QT syndrome: review of available data and practical recommendations.J Cardiovasc Electrophysiol. 2000 May;11(5):593-600. doi: 10.1111/j.1540-8167.2000.tb00015.x. J Cardiovasc Electrophysiol. 2000. PMID: 10826941 Review.
-
A patient with LQTS in whom verapamil administration and permanent pacemaker implantation were useful for preventing torsade de pointes.Pacing Clin Electrophysiol. 2004 Jan;27(1):123-4. doi: 10.1111/j.1540-8159.2004.00400.x. Pacing Clin Electrophysiol. 2004. PMID: 14720170
Cited by
-
Idiopathic short-coupled ventricular tachyarrhythmias: Systematic review and validation of electrocardiographic indices.Egypt Heart J. 2018 Dec;70(4):301-306. doi: 10.1016/j.ehj.2018.06.003. Epub 2018 Jun 22. Egypt Heart J. 2018. PMID: 30591747 Free PMC article. Review.
-
Pharmacological approach to the treatment of long and short QT syndromes.Pharmacol Ther. 2008 Apr;118(1):138-51. doi: 10.1016/j.pharmthera.2008.02.001. Pharmacol Ther. 2008. PMID: 18378319 Free PMC article. Review.
-
Arrhythmias in the congenital long QT syndrome: how often is torsade de pointes pause dependent?Heart. 2000 Jun;83(6):661-6. doi: 10.1136/heart.83.6.661. Heart. 2000. PMID: 10814624 Free PMC article. Review.
-
Identification and characterization of two novel KCNH2 mutations contributing to long QT syndrome.PLoS One. 2024 Jan 5;19(1):e0287206. doi: 10.1371/journal.pone.0287206. eCollection 2024. PLoS One. 2024. PMID: 38181028 Free PMC article.
-
Provocation of sudden heart rate oscillation with adenosine exposes abnormal QT responses in patients with long QT syndrome: a bedside test for diagnosing long QT syndrome.Eur Heart J. 2006 Feb;27(4):469-75. doi: 10.1093/eurheartj/ehi460. Epub 2005 Aug 16. Eur Heart J. 2006. PMID: 16105845 Free PMC article.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources