

Evidence for multiclonality in multicentric Kaposi's sarcoma
- PMID: 9653174
- PMCID: PMC20963
- DOI: 10.1073/pnas.95.14.8257
Evidence for multiclonality in multicentric Kaposi's sarcoma
Abstract
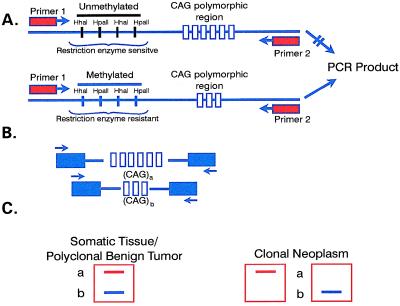
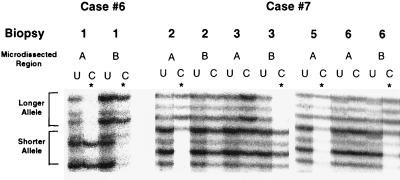
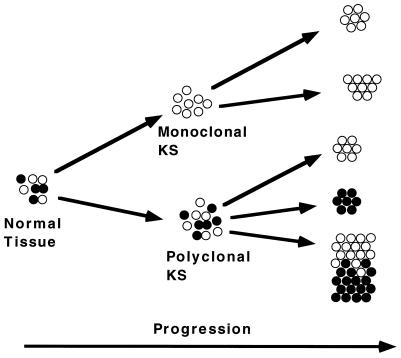
Kaposi's sarcoma (KS) develops in a variety of clinical states and is the most common tumor seen in patients with HIV-1 infection. KS develops as a multifocal mucocutaneous disease with subsequent spread to visceral organs, and it has been argued to be a benign proliferation caused by its multifocality at initial presentation, lack of aneuploidy, and spontaneous regression upon withdrawal of immunosuppressive agents in iatrogenically induced disease. We wished to determine whether KS lesions are clonal, indicative of a true neoplasm. Also, we tested whether multifocal KS lesions are clonally related, derived from a common progenitor cell or of independent cellular origin. We studied the X-chromosome inactivation pattern of the human androgen receptor gene in tumor biopsies of women with KS. This procedure tests for the clonality of a tissue specimen, a hallmark of neoplasia. Each specimen was microdissected to minimize normal cell contamination. Of 12 evaluable cases, 10 were HIV-seropositive and 2 were HIV-seronegative. Twenty-four biopsies from the 12 patients were examined. Five cases were consistent with individual KS lesions being clonal. In two cases, multiple KS specimens derived from the individual patients had different androgen receptor alleles inactivated, proving unequivocally that these KS lesions arose independently from distinct transformed cells. In seven cases, only a polyclonal pattern of inactivation was observed, whereas two others had tumor areas of both clonal and polyclonal inactivation patterns. These findings suggest that KS can be a clonal neoplasm, and in some of the cases multiple KS lesions in a given patient can arise from independent cellular origins and acquire clonal characteristics. The polyclonal inactivation pattern observed in other KS lesions may represent a premalignant stage or false negative results.
Figures
References
-
- Wahman A, Melnick S, Rhame F S, Potter J D. Epidemiol Rev. 1991;13:178–199. - PubMed
-
- Penn I. Transplantation. 1979;27:8–11. - PubMed
-
- Lifson A R, Darrow W W, Hessol N A, O’Malley P M, Barnhart L, Jaffe H J, Rutherford G W. Am J Epidemiol. 1990;131:221–231. - PubMed
-
- Gill P S, Hamilton A, Naidu Y. AIDS Updates. 1994;7:1–11.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
