

Hospital acquired native valve endocarditis: analysis of 22 cases presenting over 11 years
- PMID: 9659189
- PMCID: PMC1728707
Hospital acquired native valve endocarditis: analysis of 22 cases presenting over 11 years
Abstract
Objective: To analyse hospital acquired infective endocarditis cases with respect to age, sex, clinical, laboratory, and echocardiographic features, predisposition, complications, surgery, mortality, and diagnostic criteria.
Design: Prospective cohort study.
Setting: Teaching hospital.
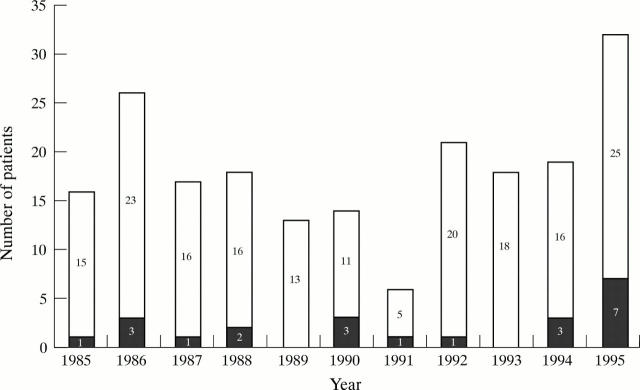
Patients: A series of 200 patients with infective endocarditis presenting over 11 years, 168 with native valve infective endocarditis, of whom 22 acquired this infection in hospital.
Results: 22 (14%) of the 168 cases of native valve infection were hospital acquired. The most common pathogens were staphylococci (77%). Two thirds of patients had no cardiac predisposition; one third had end stage renal disease. The most common source of infection was vascular access sites (73%). Eleven patients died. In 11 cases, infective endocarditis was proven pathologically (six at necropsy, five during surgery) and analysis of these showed that 45% were classed as probable by the Beth Israel criteria, 73% as definite by the Duke criteria, and 91% as definite by our suggested modifications of the Duke criteria. Figures for the 11 cases not proven pathologically were 27%, 73%, and 91%, respectively. Five of the 22 cases (22%) were rejected by the Beth Israel criteria but none were rejected by the Duke criteria with or without our modifications.
Conclusions: Hospital acquired infective endocarditis is difficult to diagnose. The Duke criteria have improved diagnostic sensitivity and our modifications have improved it further. Mortality is high but has been reduced by surgery. This serious infection could, in many cases, be prevented by improved care of intravascular lines and prompt removal when obviously infected.
Figures
Similar articles
-
Review of 65 cases of infective endocarditis in Dunedin Public Hospital.N Z Med J. 2004 Aug 20;117(1200):U1021. N Z Med J. 2004. PMID: 15475991
-
Staphylococcus aureus endocarditis at a community teaching hospital, 1980 to 1991. An analysis of 106 cases.Arch Intern Med. 1994 Oct 24;154(20):2330-5. Arch Intern Med. 1994. PMID: 7944855
-
[Trend and contributing factors of in-hospital deaths in patients with infective endocarditis over the last twenty years].J Cardiol. 2006 Feb;47(2):73-81. J Cardiol. 2006. PMID: 16515357 Japanese.
-
Endocarditis in burn patients: clinical and diagnostic considerations.Burns. 2008 Aug;34(5):610-6. doi: 10.1016/j.burns.2007.08.002. Epub 2007 Oct 29. Burns. 2008. PMID: 18029099 Review.
-
[Endocarditis caused by Staphylococcus lugdunensis. Hospital incidence].Enferm Infecc Microbiol Clin. 1998 May;16(5):233-6. Enferm Infecc Microbiol Clin. 1998. PMID: 9666587 Review. Spanish.
Cited by
-
Acp. Best practice no 155. Pathological investigation of deaths following surgery, anaesthesia, and medical procedures.J Clin Pathol. 1999 Sep;52(9):640-52. doi: 10.1136/jcp.52.9.640. J Clin Pathol. 1999. PMID: 10655984 Free PMC article. Review.
-
Right-Sided Infective Endocarditis 2020: Challenges and Updates in Diagnosis and Treatment.J Am Heart Assoc. 2020 Aug 4;9(15):e017293. doi: 10.1161/JAHA.120.017293. Epub 2020 Jul 23. J Am Heart Assoc. 2020. PMID: 32700630 Free PMC article. Review.
-
Healthcare-Associated Infective Endocarditis-Surgical Perspectives.J Clin Med. 2022 Aug 24;11(17):4957. doi: 10.3390/jcm11174957. J Clin Med. 2022. PMID: 36078887 Free PMC article. Review.
-
Health Care-Associated Infective Endocarditis: a Growing Entity that Can Be Prevented.Curr Infect Dis Rep. 2014 Nov;16(11):439. doi: 10.1007/s11908-014-0439-4. Curr Infect Dis Rep. 2014. PMID: 25230606
-
A Rare Case of Blood Culture-Negative Isolated Pulmonic Valve Endocarditis Causing Empyema.Cureus. 2022 Sep 13;14(9):e29137. doi: 10.7759/cureus.29137. eCollection 2022 Sep. Cureus. 2022. PMID: 36258987 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical