

Immunohistochemical localization of somatostatin receptors sst2A in human tumors
- PMID: 9665484
- PMCID: PMC1852945
- DOI: 10.1016/S0002-9440(10)65564-2
Immunohistochemical localization of somatostatin receptors sst2A in human tumors
Abstract
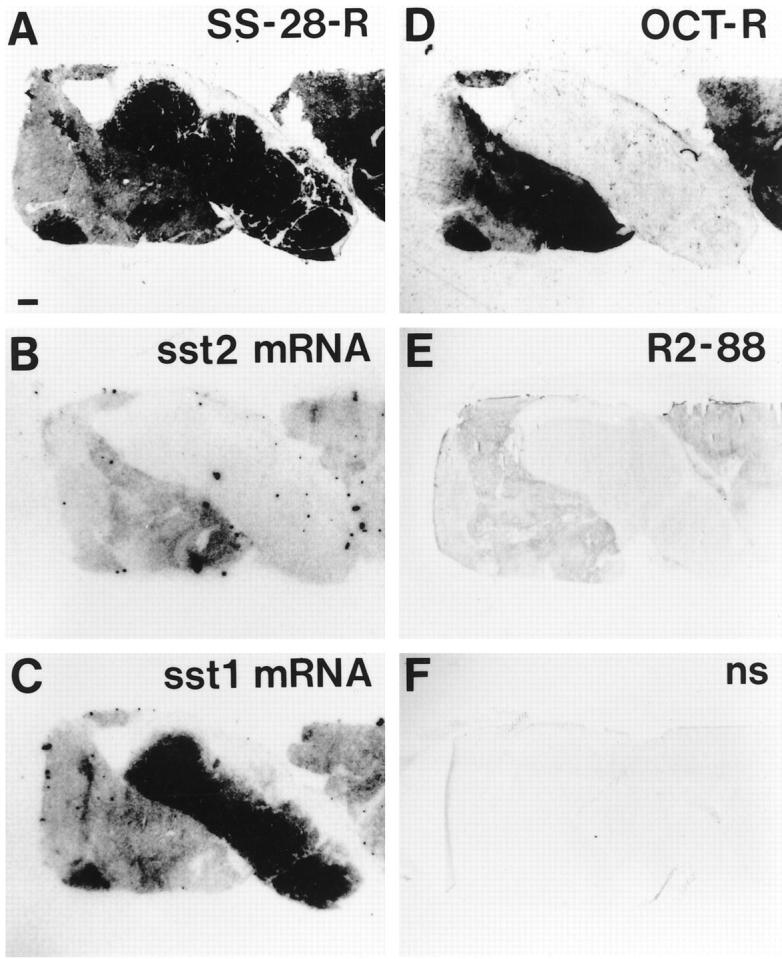
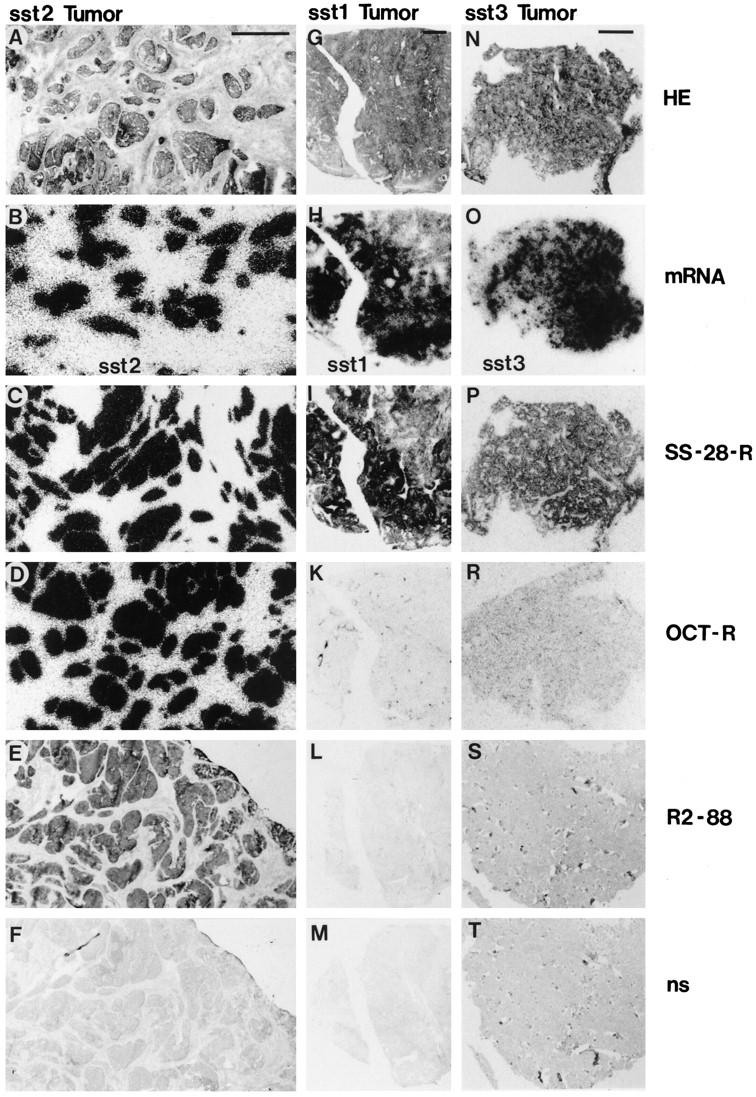
Human tumors frequently express somatostatin receptors. However, none of the receptor subtype proteins have been individually visualized in normal or neoplastic human tissues. Here, the distribution of the sst2A receptor was investigated using immunohistochemistry with the specific anti-peptide antibody R2-88 in 47 human tumors. All tumors selected for their abundance of sst2 mRNA and/or strong binding of the sst2-preferring ligand 125I-labeled Tyr3-octreotide were specifically immunostained with R2-88. Conversely, all tumors without somatostatin binding or expressing predominantly other somatostatin receptor subtype mRNAs (sst1 or sst3) were not specifically immunostained by R2-88. Specificity was shown in immunoblots, demonstrating receptor migration as a 70-kd broad band. In immunohistochemical and immunoblotting experiments, the abolition of staining after antibody blockade with antigen peptide was demonstrated. Immunostaining was identified in cryostat and in formalin-fixed, paraffin-embedded sections. Heat-induced epitope retrieval was necessary to visualize sst2A receptors in formalin-fixed sections. Moreover, because of occasional high nonspecific staining, the demonstration of complete abolition of immunostaining by treatment with antigen peptide was a prerequisite for the correct identification of sst2A-positive tumors. The sst2A receptors were clearly located at the membrane of the tumor cells. These results provide the first localization of a somatostatin receptor subtype in human tissues at the cellular level. The sst2A receptor identification and visualization in tumors with simple immunohistochemical methods in formalin-fixed, paraffin-embedded material will open new diagnostic opportunities for pathologists.
Figures






References
-
- Reubi JC: Relevance of somatostatin receptors and other peptide receptors in pathology. Endocr Pathol 1997, 8:11-20 - PubMed
-
- Krenning EP, Bakker WH, Breeman WAP, Koper JW, Kooij PPM, Ausema L, Lameris JS, Reubi JC, Lamberts SWJ: Localisation of endocrine-related tumours with radioiodinated analogue of somatostatin. Lancet 1989, I:242-244 - PubMed
-
- Lamberts SWJ, Bakker WH, Reubi JC, Krenning EP: Somatostatin-receptor imaging in the localization of endocrine tumors. N Engl J Med 1990, 323:1246-1249 - PubMed
-
- Reubi JC: Neuropeptide receptors in health and disease: the molecular basis for in vivo imaging. J Nucl Med 1995, 36:1825-1835 - PubMed
-
- Lamberts SWJ, Krenning EP, Reubi JC: The role of somatostatin and its analogs in the diagnosis and treatment of tumors. Endocr Rev 1991, 12:450-482 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
