

Onychomycosis: pathogenesis, diagnosis, and management
- PMID: 9665975
- PMCID: PMC88888
- DOI: 10.1128/CMR.11.3.415
Onychomycosis: pathogenesis, diagnosis, and management
Abstract
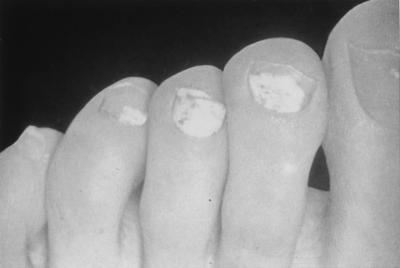
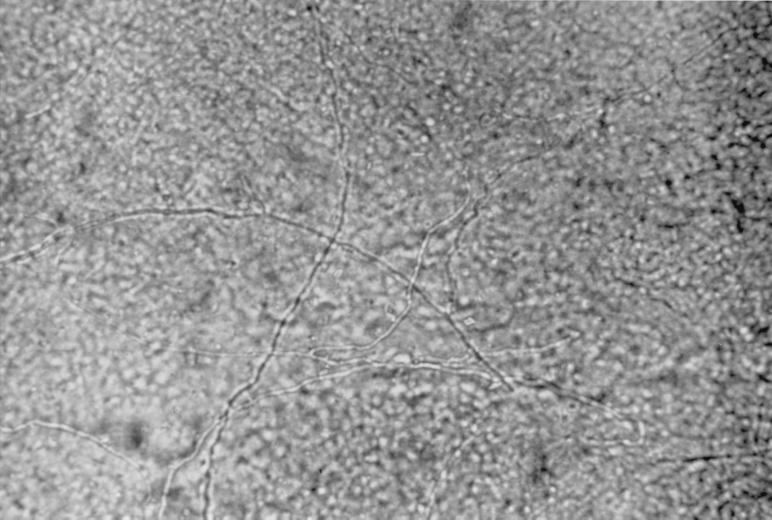
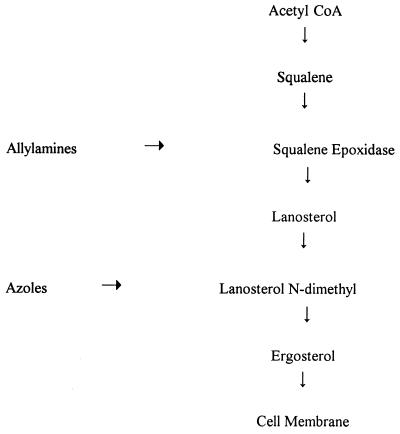
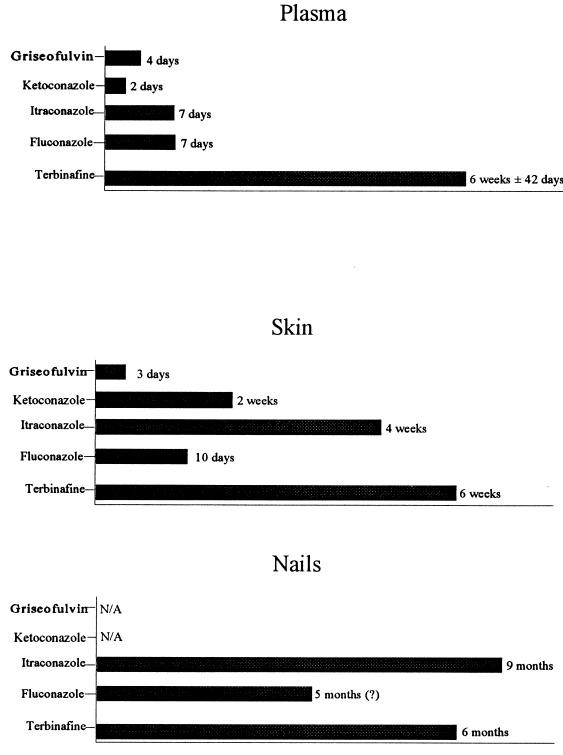
Although not life-threatening, onychomycosis (a fungal infection of the nail, usually caused by a dermatophyte) constitutes an important public health problem because of its high prevalence (about 10% of the U.S. population) and associated morbidity. The disease can have certain negative consequences for patients, such as pain, and can potentially undermine work and social lives. This review discusses the etiology, classification, diagnosis, and treatment of onychomycosis. Four types of onychomycosis are recognized based on the site and pattern of fungal invasion. Dermatophyte fungi are the predominant pathogens, but yeasts (especially Candida albicans) and nondermatophyte molds may also be implicated. Accurate diagnosis requires direct microscopy and fungal culture. The differential diagnosis includes psoriasis, lichen planus, onychogryphosis, and nail trauma. Onychomycosis is more difficult to treat than most dermatophytoses because of the inherent slow growth of the nail. Older antifungal agents (ketoconazole and griseofulvin) are unsuitable for onychomycosis because of their relatively poor efficacy and potential adverse effects. Three recently developed antimycotic agents (fluconazole, itraconazole, and terbinafine) offer high cure rates and good safety profiles. In addition, the short treatment times (< 3 months) and intermittent dosing schedules are likely to enhance compliance and reduce the costs of therapy.
Figures




References
-
- Aly R. Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol. 1994;31:S21–S25. - PubMed
-
- Aly, R., and T. Berger. 1996. Common superficial fungal infections in patients with AIDS. Clin. Infect. Dis. 22(Suppl. 2):S128–S132. - PubMed
-
- André J, Achten G. Onychomycosis. Int J Dermatol. 1987;26:481–490. - PubMed
-
- Arenas R, Dominguez-Cherit J, Fernandez L M. Open randomized comparison of itraconazole versus terbinafine in onychomycosis. Int J Dermatol. 1995;34:138–143. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
