

Chronic disease as a barrier to breast and cervical cancer screening
- PMID: 9669564
- PMCID: PMC1496963
- DOI: 10.1046/j.1525-1497.1998.00115.x
Chronic disease as a barrier to breast and cervical cancer screening
Abstract
Objective: To assess whether chronic disease is a barrier to screening for breast and cervical cancer.
Design: Structured medical record review of a retrospectively defined cohort.
Setting: Two primary care clinics of one academic medical center.
Patients: All eligible women at least 43 years of age seen during a 6-month period in each of the two study clinics (n = 1,764).
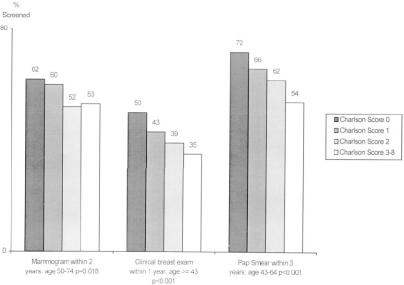
Measurements and main results: Study outcomes were whether women had been screened: for mammogram, every 2 years for ages 50-74; for clinical breast examinations (CBEs), every year for all ages; and for Pap smears, every 3 years for ages under 65. An index of comorbidity, adapted from Charlson (0 for no disease, maximum index of 8 among our patients), and specific chronic diseases were the main independent variables. Demographics, clinic use, insurance, and clinical data were covariates. In the appropriate age groups for each test, 58% of women had a mammogram, 43% had a CBE, and 66% had a Pap smear. As comorbidity increased, screening rates decreased (p < .05 for linear trend). After adjustment, each unit increase in the comorbidity index corresponded to a 17% decrease in the likelihood of mammography (p = .005), 13% decrease in CBE (p = .006), and 20% decrease in Pap smears (p = .002). The rate of mammography in women with stable angina was only two fifths of that in women without.
Conclusions: Among women who sought outpatient care, screening rates decreased as comorbidity increased. Whether clinicians and patients are making appropriate decisions about screening is not known.
Figures
Comment in
-
Screening for disease in older people.J Gen Intern Med. 1998 Jun;13(6):424-5. doi: 10.1046/j.1525-1497.1998.00126.x. J Gen Intern Med. 1998. PMID: 9669575 Free PMC article. No abstract available.
References
-
- La Vecchia C, Decarli A, Gentile A, et al. Pap smear and the risk of cervical neoplasia: quantitative estimates from a case-control study. Lancet. 1984;2:779–82. - PubMed
-
- Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL. Efficacy of screening mammography. A meta-analysis. JAMA. 1995;273(2):149–54. - PubMed
-
- US Preventive Services Task Force . Guide to Clinical Prevention Services. 2nd ed. Baltimore, Md: Williams & Wilkins; 1996.
-
- Trends in cancer screening–-United States, 1987 and 1992. MMWR. 1996;45(3):57–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials