

Pharmacokinetics, safety, and tolerability of ascending single doses of moxifloxacin, a new 8-methoxy quinolone, administered to healthy subjects
- PMID: 9687407
- PMCID: PMC105860
- DOI: 10.1128/AAC.42.8.2060
Pharmacokinetics, safety, and tolerability of ascending single doses of moxifloxacin, a new 8-methoxy quinolone, administered to healthy subjects
Abstract
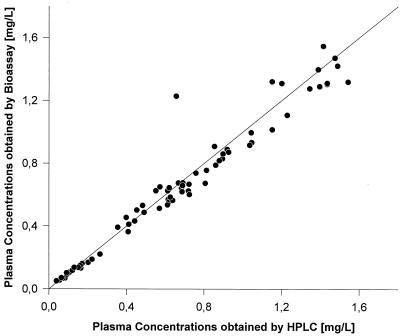
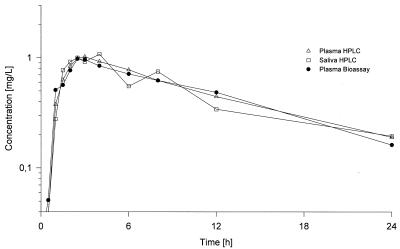
The pharmacokinetics of moxifloxacin were investigated in six studies after oral administration of 50, 100, 200, 400, 600, and 800 mg. Eight healthy male volunteers were included in each study. With doses of up to 200 mg the study was performed as a double-blind, randomized group comparison (n = 6 verum and n = 2 matched placebo); with the higher doses the study was conducted with a double-blind, randomized, crossover design. Safety and tolerability were assessed by evaluation of vital signs, electrocardiograms, electroencephalograms, clinical chemistry parameters, results of urinalysis, and adverse events. The drug was well tolerated. The concentrations of moxifloxacin in plasma, urine, and saliva were determined by a validated high-pressure liquid chromatography assay with fluorescence detection. In addition, plasma and urine samples were analyzed by a bioassay. A good correlation between both methods was seen, indicating an absence of major active metabolites. The mean maximum concentrations of moxifloxacin in plasma (Cmax) ranged from 0.29 mg/liter (50-mg dose) to 4.73 mg/liter (800-mg dose) and were reached 0.5 to 4 h following drug administration. After reaching the Cmax, plasma moxifloxacin concentrations declined in a biphasic manner. Within 4 to 5 h they fell to about 30 to 55% of the Cmax, and thereafter a terminal half-life of 11 to 14 h accounted for the major part of the area under the concentration-time curve (AUC). During the absorption phase concentrations in saliva were even higher than those in plasma, whereas in the terminal phase a constant ratio of the concentration in saliva/concentration in plasma of between 0.5 and 1 was observed, indicating a correlation between unbound concentrations in plasma and levels in saliva (protein binding level, approximately 48%). AUC and Cmax increased proportionally to the dose over the whole range of doses investigated. Urinary excretion amounted to approximately 20% of the dose. Data on renal clearance (40 to 51 ml/min/1.73 m2) indicated partial tubular reabsorption of the drug. The pharmacokinetic parameters derived from compartmental and noncompartmental analyses were in good agreement. The kinetics could be described best by fitting the data to a two-compartment body model.
Figures
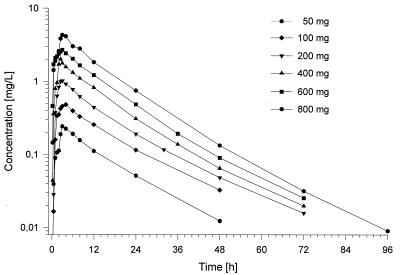
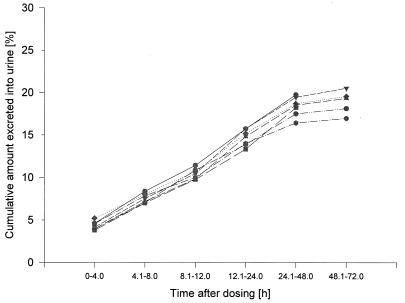
 —, 600 mg, HPLC; --—•—--, 800
mg, HPLC.
—, 600 mg, HPLC; --—•—--, 800
mg, HPLC.References
-
- Borner K, Höffken G, Lode H, Koeppe P, Prinzing C, Glätzel P, Wiley R, Olschewski P, Sievers B. Pharmacokinetics of ciprofloxacin after oral and intravenous administration. Eur J Clin Microbiol. 1986;5:179–186. - PubMed
-
- Dalhoff A, Petersen U, Endermann R. In vitro activity of BAY 12-8039, a new 8-methoxyquinolone. Chemotherapy (Basel) 1996;42:410–425. - PubMed
-
- Domdey-Bette, A. (Bayer AG). 1996. Private communication.
-
- Gibaldi M, Perrier D. Pharmacokinetics. New York, N.Y: Marcel Dekker, Inc.; 1982.
-
- Heinzel G, Woloszczak R, Thomann P. Topfit 2.0, pharmacokinetic and pharmacodynamic data analysis system for the PC. Stuttgart, Germany: Gustav Fischer; 1993.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
