

Symptoms and visceral perception in severe functional and organic dyspepsia
- PMID: 9691920
- PMCID: PMC1727129
- DOI: 10.1136/gut.42.6.814
Symptoms and visceral perception in severe functional and organic dyspepsia
Abstract
Background: Hypersensitivity of gastric afferent pathways may play an aetiological role in symptoms of functional dyspepsia.
Aims: To determine whether patients with severe organic dyspepsia (associated with tissue irritation/injury) and those with functional dyspepsia (no detectable tissue irritation) differ in their perception of gastric distension and whether this difference is reflected in differences in their gastrointestinal and psychological symptoms.
Methods: Perceptual thresholds, referral patterns, and gastrointestinal and psychological symptoms were compared in 23 patients with functional dyspepsia, 10 organic dyspeptics, and 15 healthy controls.
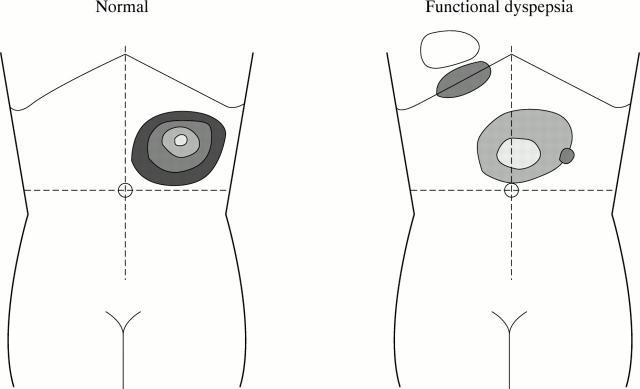
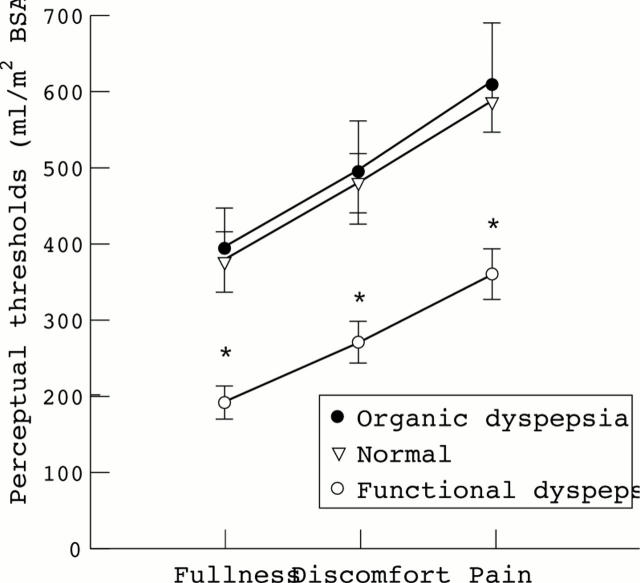
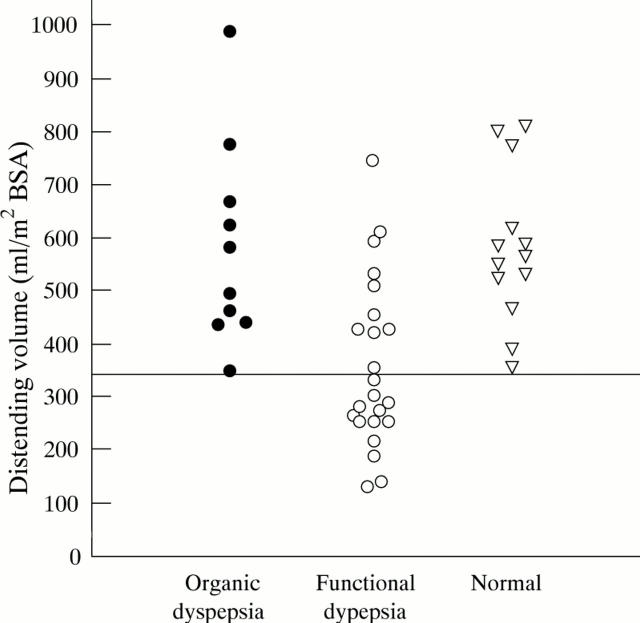
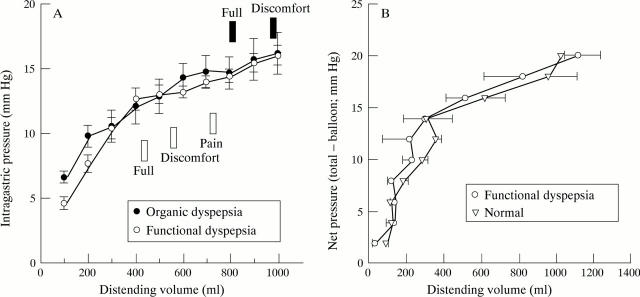
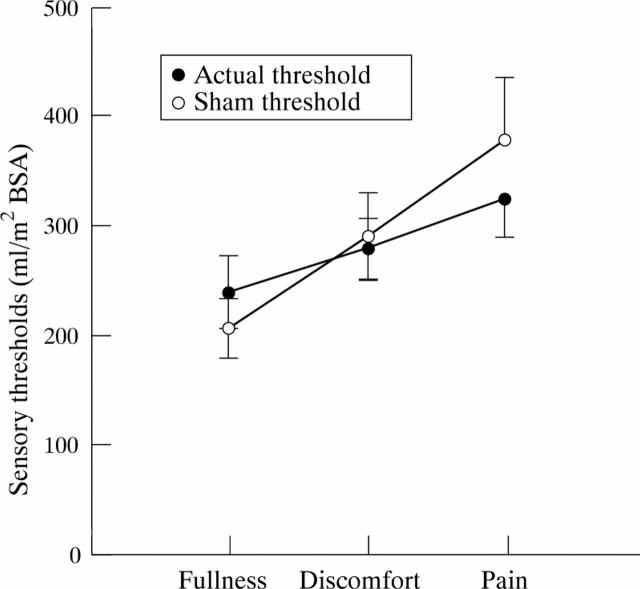
Results: Fifteen (65%) functional dyspeptics and no organic dyspeptics had reduced perceptual thresholds for fullness, discomfort, or pain (odds ratio (OR) 19.56, 95% confidence interval (CI) 1.95 to 476.09, p = 0.0017). Either reduced perceptual thresholds or altered referral was found in 20 (87%) functional dyspeptics and four (20%) organic dyspeptics (OR 10.0, 95% CI 1.34 to 89.54, p = 0.014). During sham distension fullness, discomfort and pain were reported by healthy controls, organic dyspeptics, and functional dyspeptics. A sham response of pain but no other sensation was more frequent among functional dyspeptics (43%) than healthy controls (7%) (OR 10.77, 95% CI 1.10 to 257.35, p = 0.026). Gastrointestinal and psychological symptoms and gastric compliance were similar in the functional and organic groups.
Conclusions: Alterations in the perception of gastric distension distinguishes between functional and organic dyspepsia, while symptoms do not. A total of 87% of functional dyspeptics studied had evidence of altered visceral afferent function. In this study population, psychological abnormalities or changes in compliance did not explain the findings.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical