

Initial clinical experience with the picosecond Nd:YLF laser for intraocular therapeutic applications
- PMID: 9713056
- PMCID: PMC1722590
- DOI: 10.1136/bjo.82.5.504
Initial clinical experience with the picosecond Nd:YLF laser for intraocular therapeutic applications
Abstract
Aims/background: Compared with nanosecond (ns) pulses of conventional Nd-YAG lasers, picosecond (ps) laser pulses allow intraocular surgery at considerably lower pulse energy. The authors report initial clinical experiences using a Nd:YLF ps laser for the treatment of various indications for photodisruption.
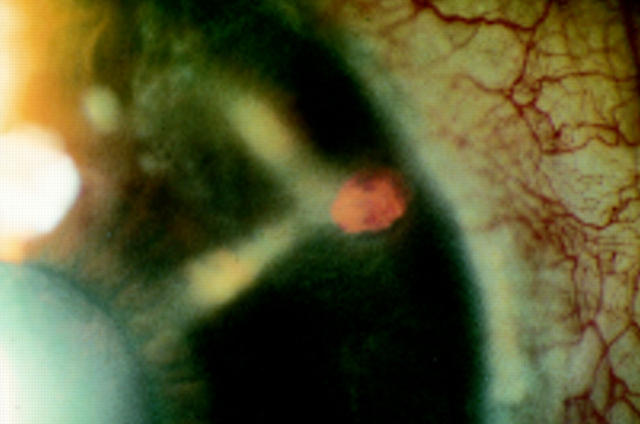
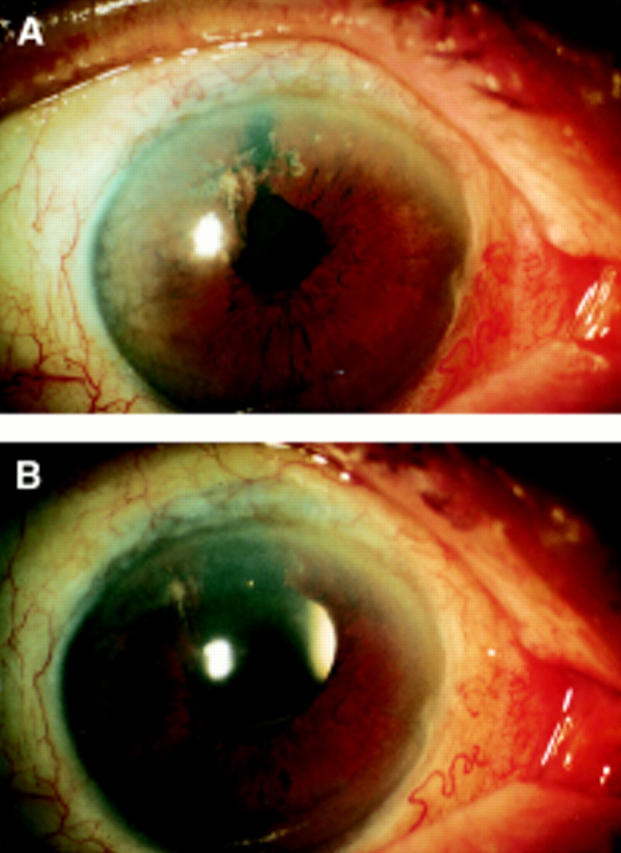
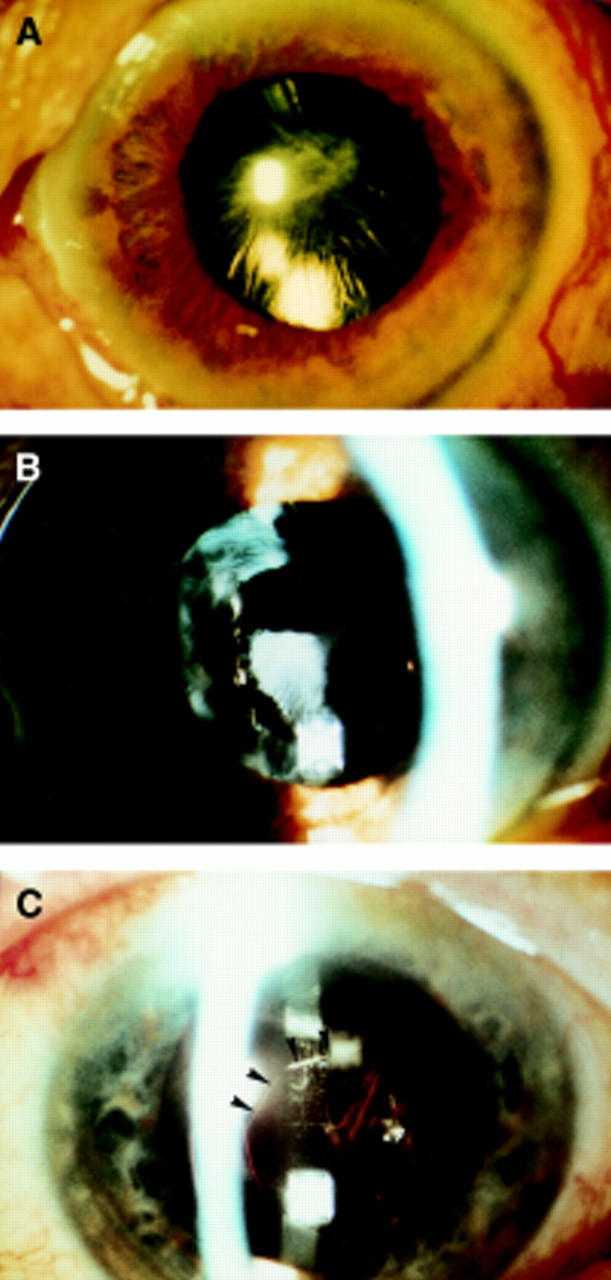
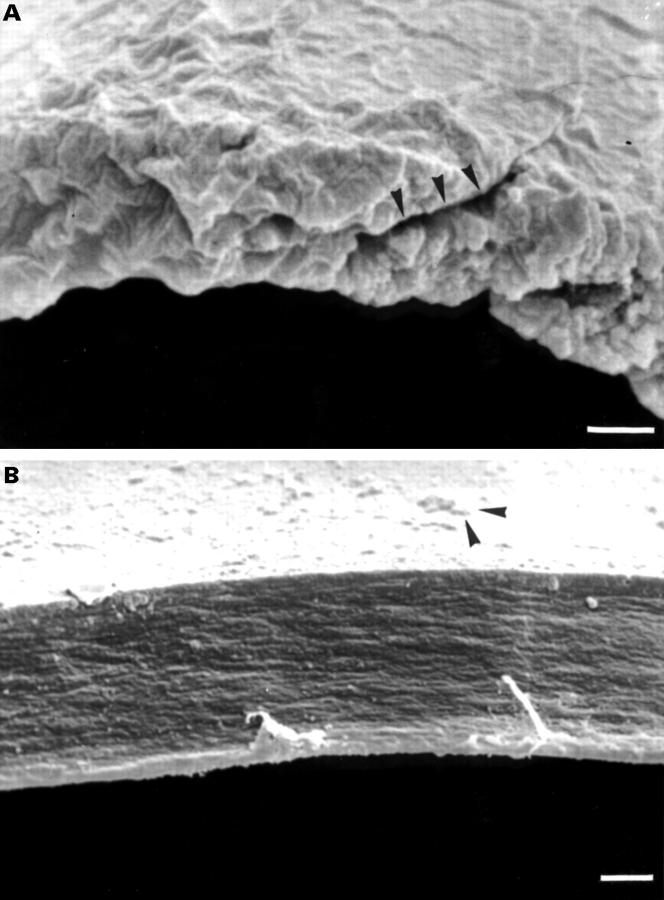
Methods: A Nd:YLF laser system (ISL 2001, wavelength 1053 nm) was used to apply pulse series of 100-400 microJ single pulse energy at a repetition rate of 0.12-1.0 kHz. Computer controlled patterns were used to perform iridectomies (n = 53), capsulotomies (n = 9), synechiolysis (n = 3), and pupilloplasties (n = 2). Other procedures were vitreoretinal strand incision (n = 2) and peripheral retinotomy (n = 1). For comparison, 10 capsulotomies and 20 iridotomies were performed with a Nd:YAG ns laser. The ps laser cut of an anterior capsule was assessed by scanning electron microscopy (SEM).
Results: Open, well defined iridectomies (mean total energy 4028 mJ, mean diameter 724 microns), were achieved at first attempt in 92% of the cases. In 64% an iris bleeding and in 21% an IOP increase of > 10 mm Hg occurred. All capsulotomies were performed successfully (mean energy 690 mJ/mm cutting length) but with a high incidence of intraocular lens damage. The attempted vitreoretinal applications remained unsuccessful as a result of optical aberrations of the eye and contact lens. Although ps laser capsulotomies and iridectomies required much higher total energy than ns procedures, the resulting tissue effects of the ps pulses were more clearly defined. SEM examination of a ps incision of the anterior lens capsule demonstrated, nevertheless, that the cut was more irregular than the edge of a continuous curvilinear capsulorhexis.
Conclusion: Series of ps pulses applied in computer controlled patterns can be used effectively for laser surgery in the anterior segment and are considerably less disruptive than ns pulses. The ps laser is well suited for laser iridectomies while the ns laser is preferable for posterior capsulotomies. As vitreoretinal applications remained unsuccessful, the range of indications for intraocular photodisruption could not be extended by the ps laser.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous