

Development of specific immunoglobulins G, M, and A following primary Toxoplasma gondii infection in pregnant women
- PMID: 9738042
- PMCID: PMC105086
- DOI: 10.1128/JCM.36.10.2907-2913.1998
Development of specific immunoglobulins G, M, and A following primary Toxoplasma gondii infection in pregnant women
Abstract
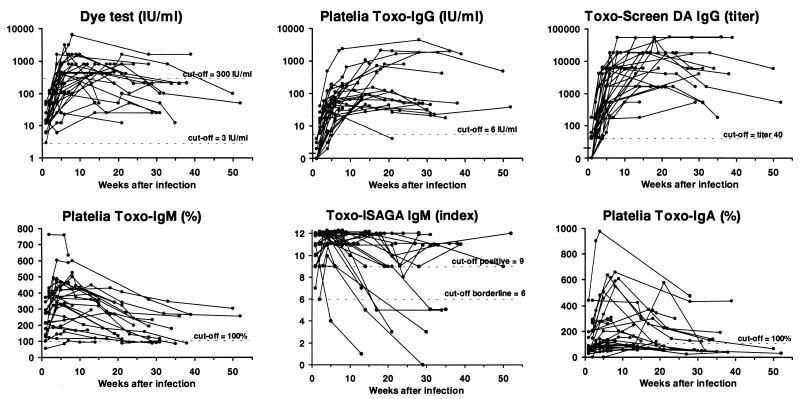
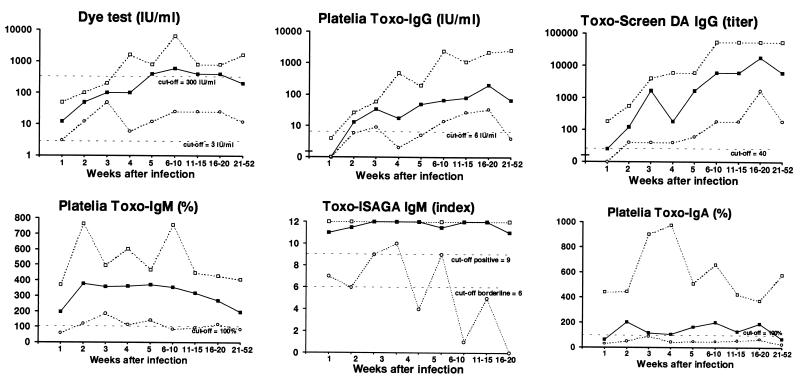
The development of specific antibodies following primary Toxoplasma gondii infection during pregnancy was assessed by six different antibody assays: dye test, Platelia Toxo-IgG, Toxo-Screen DA IgG, Platelia Toxo-IgM, Toxo-ISAGA IgM, and Platelia Toxo-IgA. A total of 126 sera from 27 pregnant women, for whom the time of acquisition of infection could be estimated fairly accurately, were included. All tests showed great individual variation in the peak amounts of antibodies detected. The times elapsed after infection until the peak was reached also varied greatly from individual to individual: the ranges were 2 to 21 weeks for the dye test, 4 to 36 weeks for Platelia Toxo-IgG, 4 to 30 weeks for Toxo-Screen DA IgG, 2 to 18 weeks for Platelia Toxo-IgM, 1 to 6 weeks for Toxo-ISAGA IgM, and 2 to 21 weeks for Platelia Toxo-IgA. In the early phase of the infection the dye test and the specific-IgM tests were the most sensitive. Toxo-Screen DA IgG was more sensitive than Platelia Toxo-IgG in the acute phase, while Platelia Toxo-IgA was clearly the least sensitive assay. Of the sera collected 21 to 52 weeks after infection, all were positive by the dye test, all except one (which was negative by Platelia Toxo-IgG) were positive by the specific-IgG tests, approximately 80% were positive by the IgM tests, and 45% were positive by the IgA test. Due to the great individual variation it seems impossible to estimate when the infection occurred based on results obtained from a single serum, and it may even be difficult to assess when a titer increase in paired sera is detectable unless the first sample is only marginally positive. As a diagnostic criterion a dye test titer of >/=300 IU/ml has a low sensitivity for recent primary infection.
Figures
References
-
- Aspöck H, Pollak A. Prevention of prenatal toxoplasmosis by serological screening of pregnant women in Austria. Scand J Infect Dis Suppl. 1992;84:32–37. - PubMed
-
- Benenson M W, Takafuji E T, Lemon S M, Greenup R L, Sulzer A J. Oocyst-transmitted toxoplasmosis associated with ingestion of contaminated water. N Engl J Med. 1982;307:666–669. - PubMed
-
- Beverly J K A, Beattie C P. Glandular toxoplasmosis. A survey of 30 cases. Lancet. 1958;ii:379–384. - PubMed
-
- Brooks R G, McCabe R E, Remington J S. Role of serology in the diagnosis of toxoplasma lymphadenopathy. Rev Infect Dis. 1987;9:1055–1062. - PubMed
-
- Cesbron J Y, Capron A, Ovlaque G, Santoro F. Use of monoclonal antibody in a double sandwich ELISA for detection of IgM antibodies to Toxoplasma gondii major surface protein (P30) J Immunol Methods. 1985;83:151–158. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
