

A multidisciplinary approach for improving services in primary care: randomised controlled trial of screening for haemoglobin disorders
- PMID: 9740569
- PMCID: PMC28672
- DOI: 10.1136/bmj.317.7161.788
A multidisciplinary approach for improving services in primary care: randomised controlled trial of screening for haemoglobin disorders
Abstract
Objective: To investigate the feasibility of improving screening for carriers of haemoglobin disorders in general practice by using a nurse facilitator to work with primary care teams and the relevant haematology laboratories; to identify problems in communication between all those involved in delivering the service, and to implement solutions.
Design: Two year, practice based randomised controlled trial.
Setting: North London area where 29% of residents and 43% of births are in ethnic groups at risk for haemoglobin disorders.
Subjects: 26 of the 93 practices using the services of the area's haematology laboratory agreed to take part and were randomly divided into control and intervention practices.
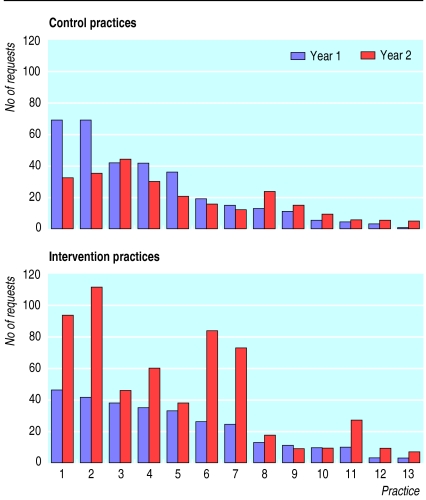
Main outcome measure: Change in number of requests for screening tests for haemoglobin disorders made by control and intervention practices in baseline and intervention years.
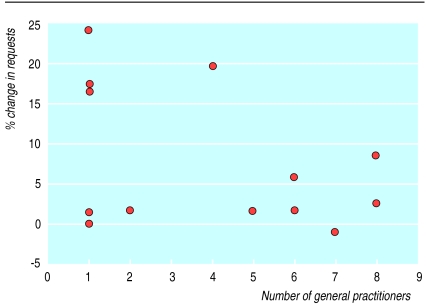
Results: The number of screening tests requested varied from 0-150 in the 93 practices in the baseline year. Study practices tended to have made a moderate number of requests (10-50) during this period. During the intervention year intervention practices made 292 more requests (99% increase) and control practices made 74 fewer requests (23% decrease; P=0.001 for difference in median change). Four practices, three of which were singlehanded, accounted for 75% of the increase. The number of requests from intervention practices, adjusted for baseline requests, was 3.2 times higher than control practices (P<0.0001).
Conclusion: General practitioners and practice nurses are willing to undertake a new genetic screening service (or expand an existing one) if they are persuaded that it benefits the health of a significant proportion of their practice population. They need appropriate tools (for example, information materials for carriers and groups at risk), and the laboratory must be sensitive to their needs. Preconceptional carrier screening and counselling need to be coupled with antenatal screening.
Figures
Comment in
-
Thalassaemia among Asians in Britain. Thalassaemia Society is working to improve awareness.BMJ. 1999 Mar 27;318(7187):873. doi: 10.1136/bmj.318.7187.873. BMJ. 1999. PMID: 10092276 Free PMC article. No abstract available.
References
-
- Department of Health. Report of a Working Party of the Standing Medical Advisory Committee on Sickle Cell, Thalassaemia and other Haemoglobinopathies. London: HMSO.; 1993.
-
- Health Education Authority. Sickle cell and thalassaemia: achieving health gain—guidance for commissioners and providers. London: HEA; 1998.
-
- British Society For Haematology. Guidelines for haemoglobinopathy screening. Clin Labor Haematol. 1988;10:87–94. - PubMed
-
- Angastiniotis MA, Kyriakidou S, Hadjiminas M. How thalassaemia was controlled in Cyprus. World Health Forum. 1986;7:291–297.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources