

Should inhaled anticholinergics be added to beta2 agonists for treating acute childhood and adolescent asthma? A systematic review
- PMID: 9765164
- PMCID: PMC28680
- DOI: 10.1136/bmj.317.7164.971
Should inhaled anticholinergics be added to beta2 agonists for treating acute childhood and adolescent asthma? A systematic review
Abstract
Objectives: To estimate the therapeutic and adverse effects of addition of inhaled anticholinergics to beta2 agonists in acute asthma in children and adolescents.
Design: Systematic review of randomised controlled trials of children and adolescents taking beta2 agonists for acute asthma with or without the addition of inhaled anticholinergics.
Main outcome measures: Hospital admission, pulmonary function tests, number of nebulised treatments, relapse, and adverse effects.
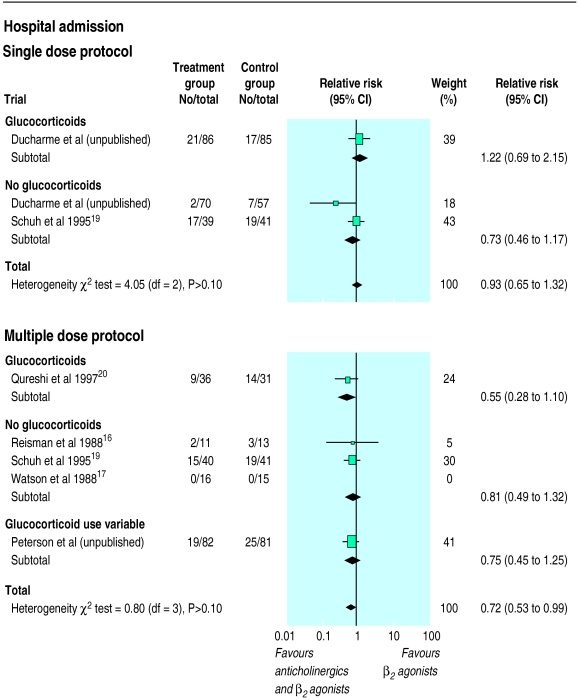
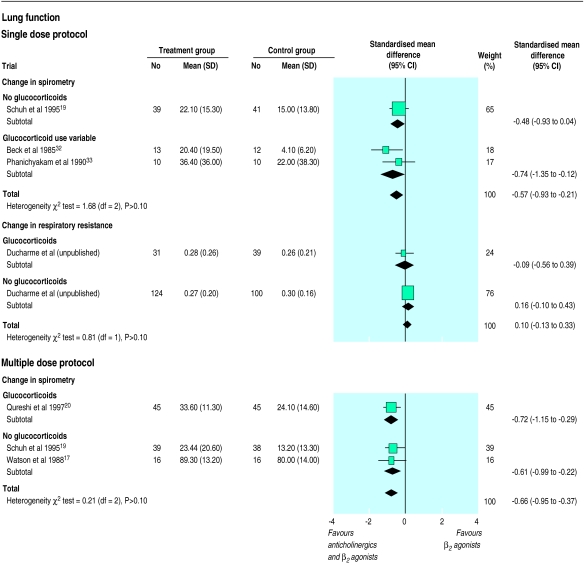
Results: Of 37 identified trials, 10 were relevant and six of these were of high quality. The addition of a single dose of anticholinergic to beta2 agonist did not reduce hospital admission (relative risk 0.93, 95% confidence interval 0.65 to 1.32). However, significant group differences in lung function supporting the combination treatment were observed 60 minutes (standardised mean difference -0.57, -0.93 to -0.21) and 120 minutes (-0.53, -0.90 to -0.17) after the dose of anticholinergic. In contrast, the addition of multiple doses of anticholinergics to beta2 agonists, mainly in children and adolescents with severe exacerbations, reduced the risk of hospital admission by 30% (relative risk 0.72, 0.53 to 0.99). Eleven (95% confidence interval 5 to 250) children would need to be treated to avoid one admission. A parallel improvement in lung function (standardised mean difference -0.66, -0.95 to -0.37) was noted 60 minutes after the last combined inhalation. In the single study where anticholinergics were systematically added to every beta2 agonist inhalation, irrespective of asthma severity, no group differences were observed for the few available outcomes. There was no increase in the amount of nausea, vomiting, or tremor in patients treated with anticholinergics.
Conclusions: Adding multiple doses of anticholinergics to beta2 agonists seems safe, improves lung function, and may avoid hospital admission in 1 of 11 such treated patients. Although multiple doses should be preferred to single doses of anticholinergics, the available evidence only supports their use in school aged children and adolescents with severe asthma exacerbation.
Figures
Comment in
-
Ipratropium does indeed reduce admissions to hospital with severe asthma.BMJ. 1999 Mar 13;318(7185):738. doi: 10.1136/bmj.318.7185.738. BMJ. 1999. PMID: 10074041 Free PMC article. No abstract available.