

Partial inactivation of the primary motor cortex hand area: effects on individuated finger movements
- PMID: 9787008
- PMCID: PMC6793546
- DOI: 10.1523/JNEUROSCI.18-21-09038.1998
Partial inactivation of the primary motor cortex hand area: effects on individuated finger movements
Abstract
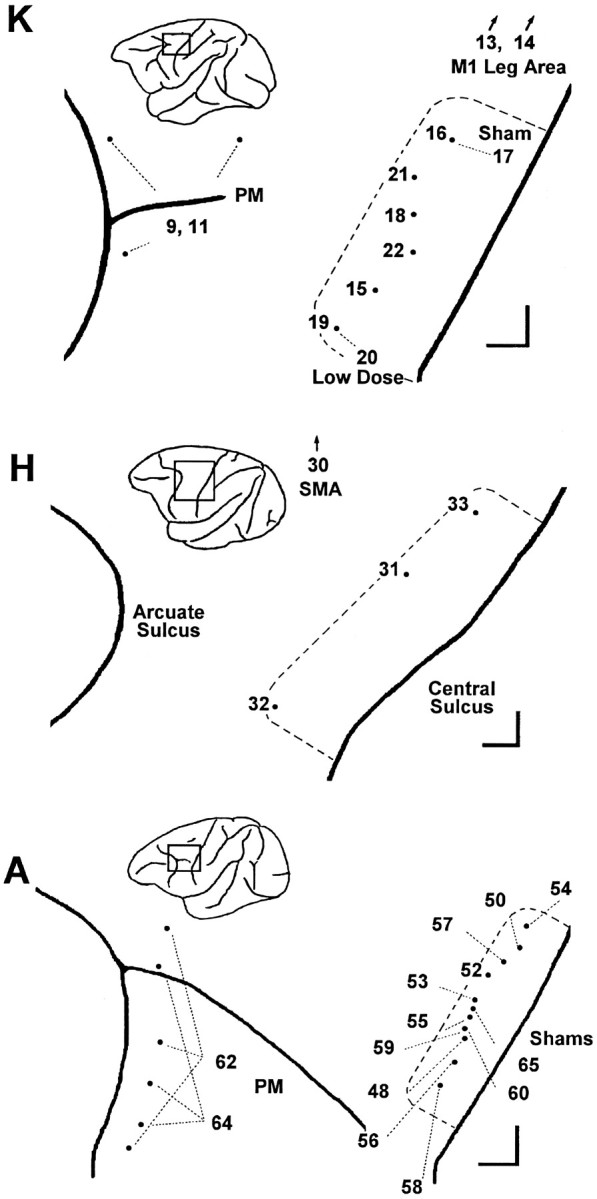
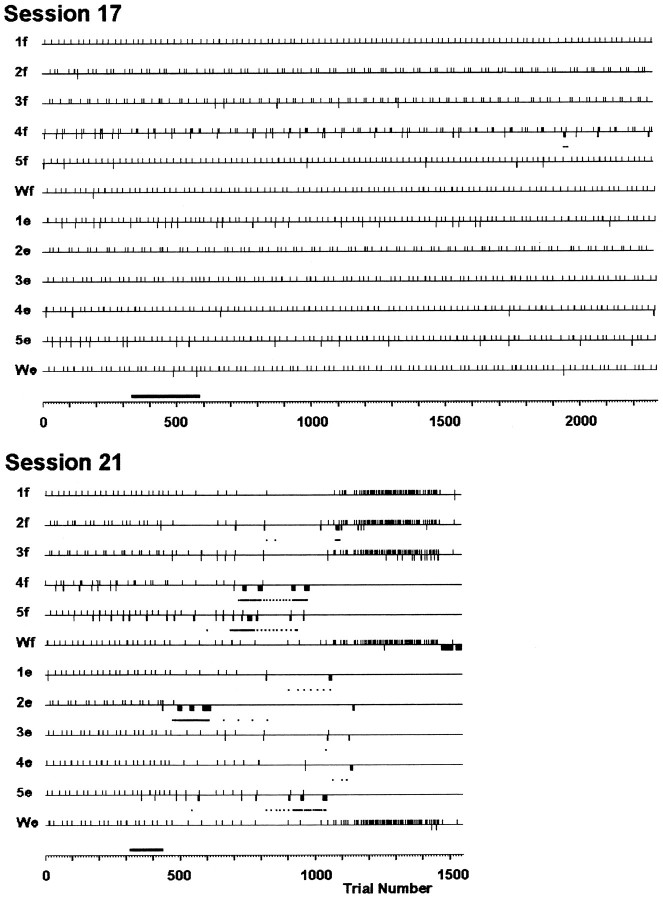
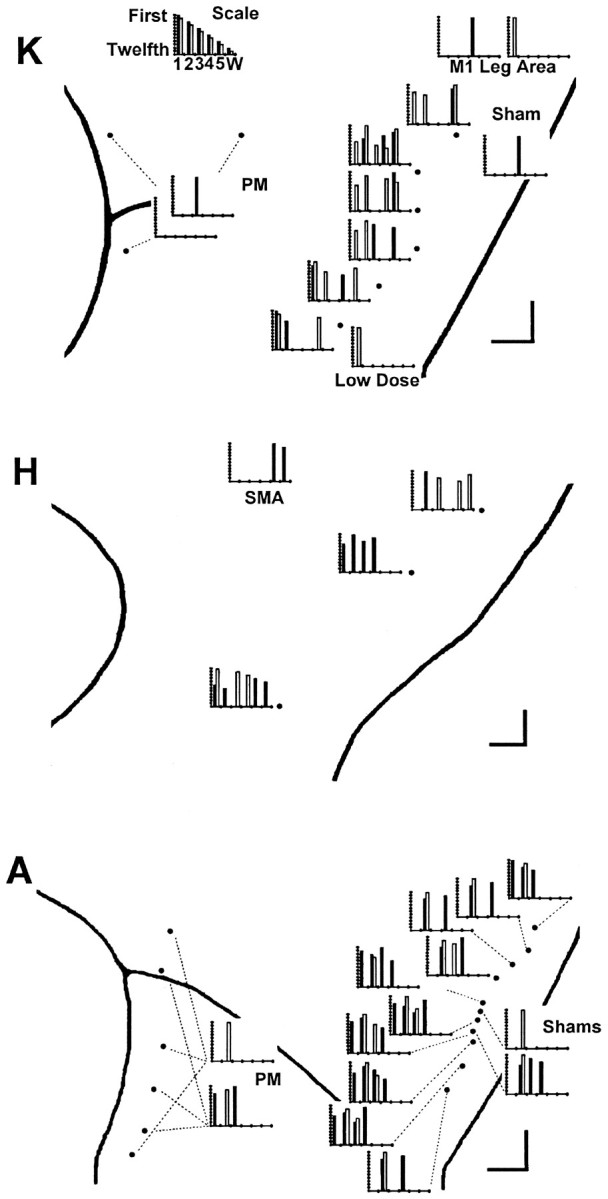
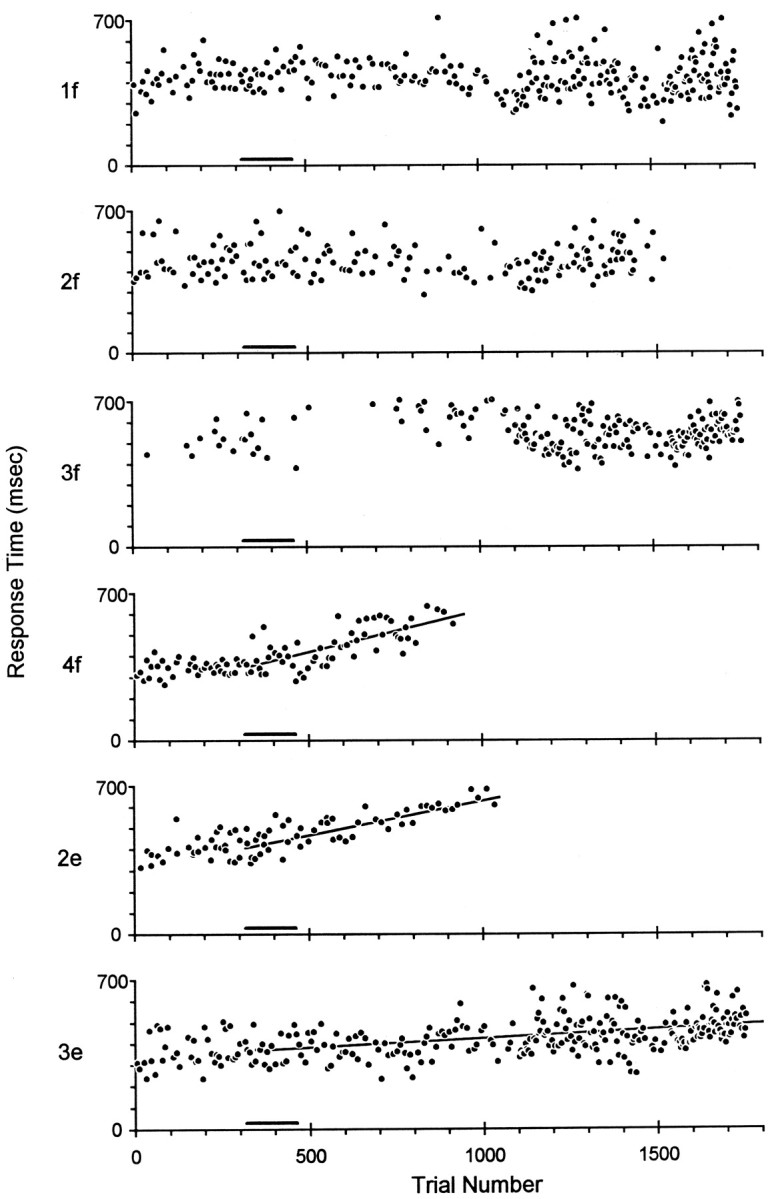
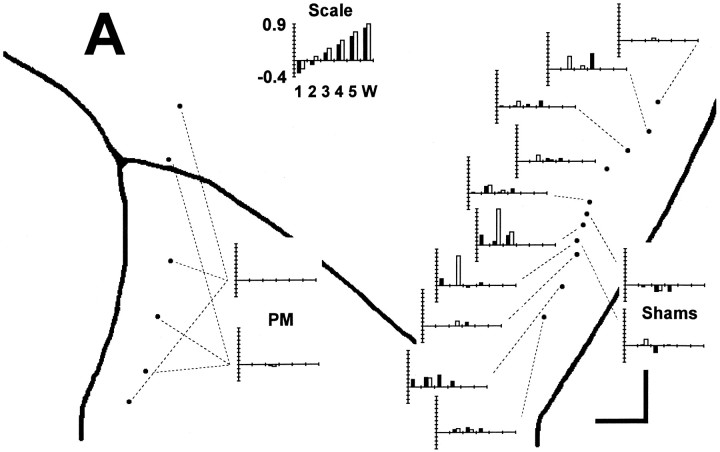
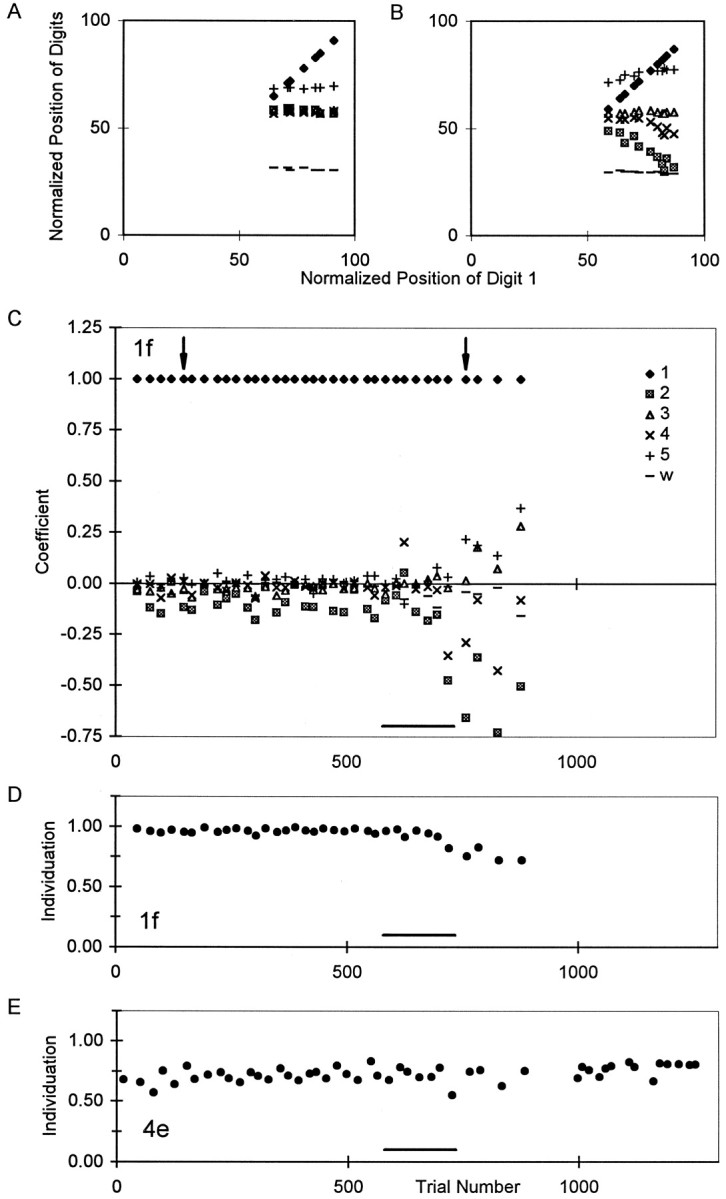
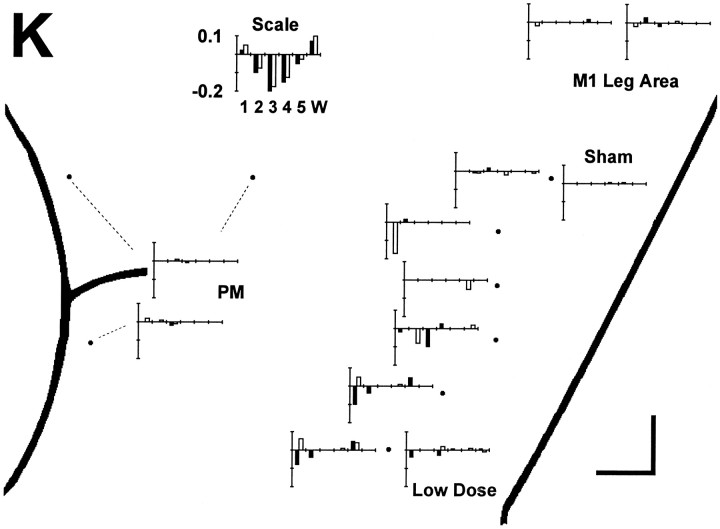
After large lesions of the primary motor cortex (M1), voluntary movements of affected body parts are weak and slow. In addition, the relative independence of moving one body part without others is lost; attempts at individuated movements of a given body part are accompanied by excessive, unintended motion of contiguous body parts. The effects of partial inactivation of the M1 hand area are comparatively unknown, however. If the M1 hand area contains the somatotopically ordered finger representations implied by the classic homunculus or simiusculus, then partial inactivation might produce weakness, slowness, and loss of independence of one or two adjacent digits without affecting other digits. But if control of each finger movement is distributed in the M1 hand area as many studies suggest, then partial inactivation might produce dissociation of weakness, slowness, and relative independence of movement, and which fingers movements are impaired might be unrelated to the location of the inactivation along the central sulcus. To investigate the motoric deficits resulting from partial inactivation of the M1 hand area, we therefore made single intracortical injections of muscimol as trained monkeys performed visually cued, individuated flexion-extension movements of the fingers and wrist. We found little if any evidence that which finger movements were impaired after each injection was related to the injection location along the central sulcus. Unimpaired fingers could be flanked on both sides by impaired fingers, and the flexion movements of a given finger could be unaffected even though the extension movements were impaired, or vice versa. Partial inactivation also could produce dissociated weakness and slowness versus loss of independence in a given finger movement. These findings suggest that control of each individuated finger movement is distributed widely in the M1 hand area.
Figures
Similar articles
-
Motor cortex and the distributed anatomy of finger movements.Adv Exp Med Biol. 2002;508:411-6. doi: 10.1007/978-1-4615-0713-0_46. Adv Exp Med Biol. 2002. PMID: 12171137
-
Decoding individuated finger movements using volume-constrained neuronal ensembles in the M1 hand area.IEEE Trans Neural Syst Rehabil Eng. 2008 Feb;16(1):15-23. doi: 10.1109/TNSRE.2007.916269. IEEE Trans Neural Syst Rehabil Eng. 2008. PMID: 18303801 Free PMC article.
-
Structure of Population Activity in Primary Motor Cortex for Single Finger Flexion and Extension.J Neurosci. 2020 Nov 25;40(48):9210-9223. doi: 10.1523/JNEUROSCI.0999-20.2020. Epub 2020 Oct 21. J Neurosci. 2020. PMID: 33087474 Free PMC article.
-
Selective activation of human finger muscles after stroke or amputation.Adv Exp Med Biol. 2009;629:559-75. doi: 10.1007/978-0-387-77064-2_30. Adv Exp Med Biol. 2009. PMID: 19227521 Free PMC article. Review.
-
Hand function: peripheral and central constraints on performance.J Appl Physiol (1985). 2004 Jun;96(6):2293-300. doi: 10.1152/japplphysiol.01063.2003. J Appl Physiol (1985). 2004. PMID: 15133016 Review.
Cited by
-
Local field potentials in primate motor cortex encode grasp kinetic parameters.Neuroimage. 2015 Jul 1;114:338-55. doi: 10.1016/j.neuroimage.2015.04.008. Epub 2015 Apr 11. Neuroimage. 2015. PMID: 25869861 Free PMC article.
-
Pronounced reduction of digit motor responses evoked from macaque ventral premotor cortex after reversible inactivation of the primary motor cortex hand area.J Neurosci. 2008 May 28;28(22):5772-83. doi: 10.1523/JNEUROSCI.0944-08.2008. J Neurosci. 2008. PMID: 18509039 Free PMC article.
-
Brain repair after stroke--a novel neurological model.Nat Rev Neurol. 2013 Dec;9(12):698-707. doi: 10.1038/nrneurol.2013.222. Epub 2013 Nov 12. Nat Rev Neurol. 2013. PMID: 24217509 Free PMC article. Review.
-
The Effects of Sex Hormonal Fluctuations during Menstrual Cycle on Cortical Excitability and Manual Dexterity (a Pilot Study).PLoS One. 2015 Aug 26;10(8):e0136081. doi: 10.1371/journal.pone.0136081. eCollection 2015. PLoS One. 2015. PMID: 26308341 Free PMC article.
-
Optimizing shoulder elevation assist rate in exoskeletal rehabilitation based on muscular activity indices: a clinical feasibility study.BMC Neurol. 2024 May 9;24(1):144. doi: 10.1186/s12883-024-03651-x. BMC Neurol. 2024. PMID: 38724916 Free PMC article.
References
-
- Andersen P, Hagan PJ, Phillips CG, Powell TP. Mapping by microstimulation of overlapping projections from area 4 to motor units of the baboon’s hand. Proc R Soc Lond B Biol Sci. 1975;188:31–36. - PubMed
-
- Ashe J. Force and the motor cortex. Behav Brain Res. 1997;86:1–15. - PubMed
-
- Beck CH, Chambers WW. Speed, accuracy, and strength of forelimb movement after unilateral pyramidotomy in rhesus monkeys. J Comp Physiol Psychol. 1970;70:1–22. - PubMed
-
- Beevor C. The Croonian Lectures on muscular movements. MacMillan; New York: 1903a. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources