

The effectiveness of cost-effectiveness analysis in containing costs
- PMID: 9798812
- PMCID: PMC1500894
- DOI: 10.1046/j.1525-1497.1998.00201.x
The effectiveness of cost-effectiveness analysis in containing costs
Abstract
Objective: Although cost-effectiveness analyses (CEAs) have been advocated as a tool to critically appraise the value of health expenditures, it has been widely hoped that they might also help contain health care costs. To determine how often they discourage additional expenditures, we reviewed the conclusions of recently published CEAs.
Data sources: A search of the Abridged Index Medicus (a subset of MEDLINE designed to afford rapid access to the literature of "immediate interest" to the practicing physician) between 1990 and 1996.
Study selection: We only included articles that reported an explicit cost-effectiveness (CE) ratio (a cost for some given health effect) in the abstract.
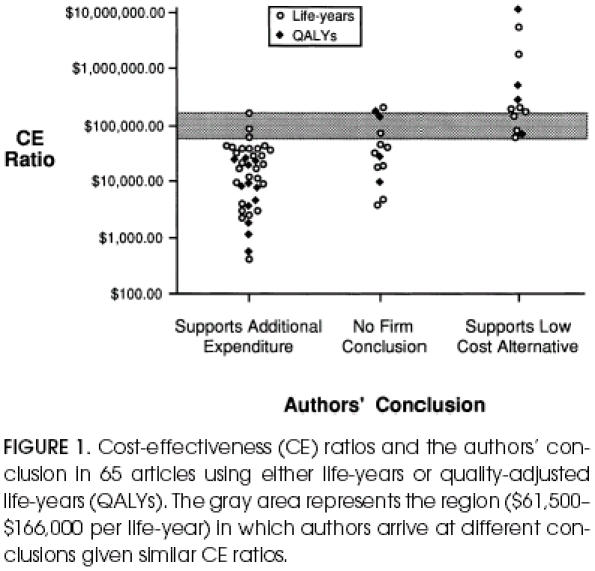
Data abstraction: From each abstract, we collected the value for the incremental CE ratio and the measure of health effect (life-years, quality-adjusted life-years [QALYs], other). We then categorized the authors' conclusion into one of three categories: supports strategy requiring additional expenditure, no firm conclusion, and supports low-cost alternative. Finally, we obtained the article and collected information on funding source.
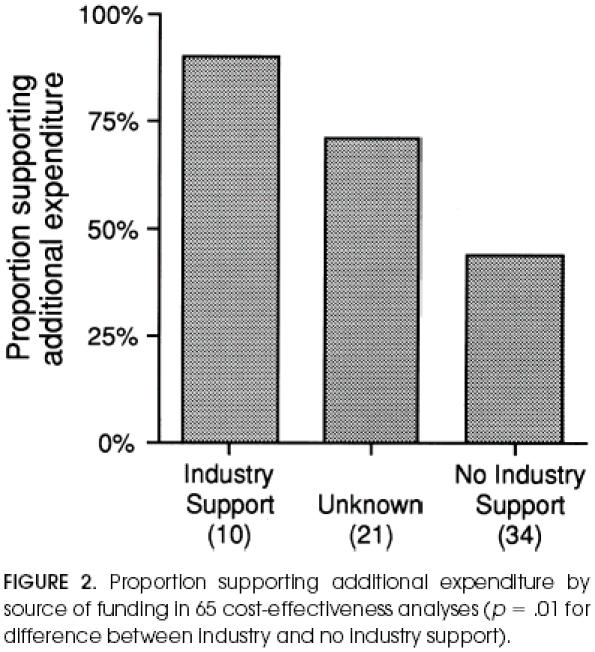
Data synthesis: Among the 109 eligible articles, the authors' conclusion supported strategies requiring additional expenditure in 58 (53%) and supported the low-cost alternative in 28 (26%). We then focused on the 65 articles reporting either life-years or QALYs. Cost-effectiveness ratios ranged from $400 to $166,000 (per life-year or QALY) in the 39 articles (60%) in which authors supported additional expenditure, and ranged from $61,500 to $11,600,000 in the 13 articles (20%) in which authors supported the low-cost alternative. Despite identifying similar CE ratios, authors arrived at different conclusions in the overlapping range ($61,500 to $166,000). Of the 10 articles acknowledging industry funding, 9 supported a strategy requiring additional expenditure (p = .01 as compared with those without such funding).
Conclusions: Authors of CEAs are more likely to support strategies requiring additional expenditure than the low-cost alternative. There is no obvious consensus about how small the CE ratio should be to warrant additional expenditure. Finally, concerns about funding source seem to be warranted.
Figures
Comment in
-
Interpretation of cost-effectiveness analyses.J Gen Intern Med. 1998 Oct;13(10):716-7. doi: 10.1046/j.1525-1497.1998.00211.x. J Gen Intern Med. 1998. PMID: 9798822 Free PMC article. Review. No abstract available.
Similar articles
-
Quality-adjusted life-years lack quality in pediatric care: a critical review of published cost-utility studies in child health.Pediatrics. 2005 May;115(5):e600-14. doi: 10.1542/peds.2004-2127. Pediatrics. 2005. PMID: 15867026 Review.
-
Costing and perspective in published cost-effectiveness analysis.Med Care. 2009 Jul;47(7 Suppl 1):S28-32. doi: 10.1097/MLR.0b013e31819bc09d. Med Care. 2009. PMID: 19536023
-
Statistical primer: a cost-effectiveness analysis.Eur J Cardiothorac Surg. 2018 Aug 1;54(2):209-213. doi: 10.1093/ejcts/ezy187. Eur J Cardiothorac Surg. 2018. PMID: 29726940
-
Cost-effectiveness of embryo transfer strategies: a decision analytic model using long-term costs and consequences of singletons and multiples born as a consequence of IVF.Hum Reprod. 2016 Nov;31(11):2527-2540. doi: 10.1093/humrep/dew229. Epub 2016 Oct 6. Hum Reprod. 2016. PMID: 27907897
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
Cost-effectiveness of Osimertinib in activating epidermal growth factor receptor gene (EGFR)-mutations in first-line for advanced non-small cell lung cancer.Cancer Drug Resist. 2021 Apr 27;4(3):740-744. doi: 10.20517/cdr.2021.14. eCollection 2021. Cancer Drug Resist. 2021. PMID: 35582308 Free PMC article. No abstract available.
-
Factors influencing medical expenditures in patients with unresolved facial palsy and pharmacoeconomic analysis of upper eyelid lid loading with gold and platinum weights compared to tarsorrhaphy.Health Econ Rev. 2024 Apr 27;14(1):30. doi: 10.1186/s13561-024-00506-6. Health Econ Rev. 2024. PMID: 38676777 Free PMC article.
-
Sequencing Systemic Therapy Pathways for Advanced Hepatocellular Carcinoma: A Cost Effectiveness Analysis.Liver Cancer. 2020 Sep;9(5):549-562. doi: 10.1159/000508485. Epub 2020 Aug 12. Liver Cancer. 2020. PMID: 33083280 Free PMC article.
-
First-line systemic treatment strategies for unresectable hepatocellular carcinoma: A cost-effectiveness analysis.PLoS One. 2023 Apr 13;18(4):e0279786. doi: 10.1371/journal.pone.0279786. eCollection 2023. PLoS One. 2023. PMID: 37053300 Free PMC article.
-
A Systematic Review of the Level of Evidence in Economic Evaluations of Medical Devices: The Example of Vertebroplasty and Kyphoplasty.PLoS One. 2015 Dec 10;10(12):e0144892. doi: 10.1371/journal.pone.0144892. eCollection 2015. PLoS One. 2015. PMID: 26661078 Free PMC article.
References
-
- Detsky AS, Naglie G. A clinician's guide to cost-effectiveness analysis. Ann Intern Med. 1990;113:147–54. - PubMed
-
- Eddy DM. Oregon's methods: did cost-effectiveness fail? JAMA. 1991;266:2135–41. - PubMed
-
- Eddy DM. Cost-effectiveness analysis: a conversation with my father. JAMA. 1992;267:1669–75. - PubMed
-
- Thompson MS. Beverly Hills: Calif: Sage;; 1980. Benefit-cost analysis for program evaluation.
-
- Warner KE, Hutton RC. Cost benefit and cost-effectiveness analysis in health care. Med Care. 1980;18:1060–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources