

Survival after in-hospital cardiopulmonary resuscitation. A meta-analysis
- PMID: 9844078
- PMCID: PMC1497044
- DOI: 10.1046/j.1525-1497.1998.00244.x
Survival after in-hospital cardiopulmonary resuscitation. A meta-analysis
Abstract
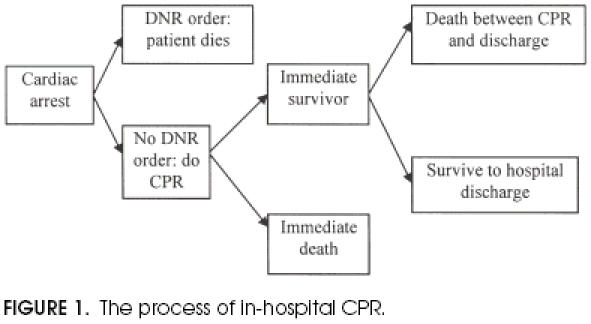
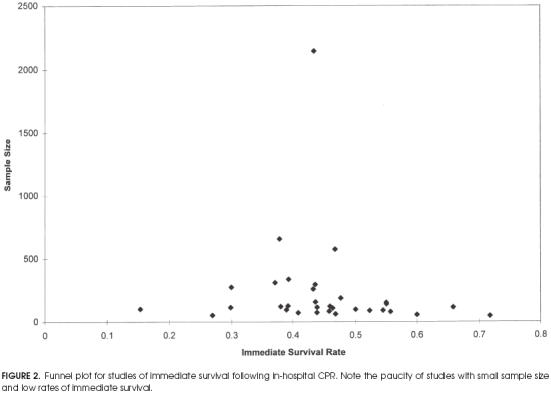
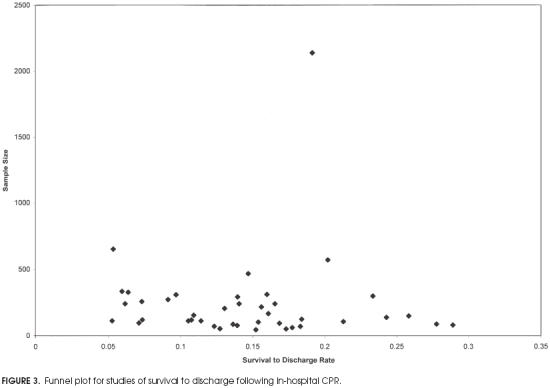
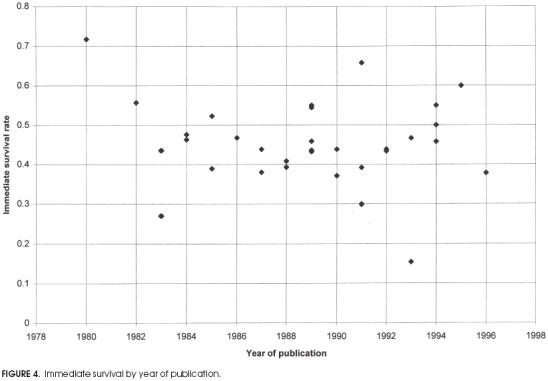
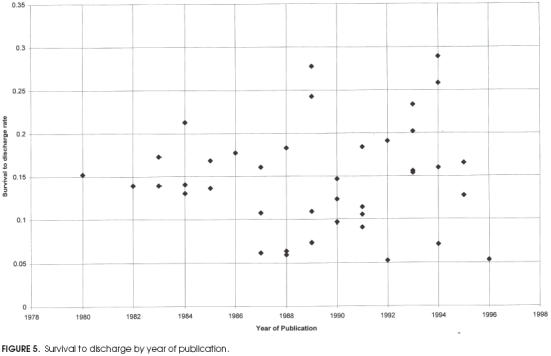
Objective: To determine the rates of immediate survival and survival to discharge for adult patients undergoing in-hospital cardiopulmonary resuscitation, and to identify demographic and clinical variables associated with these outcomes.
Measurements and main results: The MEDLARS database of the National Library of Medicine was searched. In addition, the authors' extensive personal files and the bibliography of each identified study were searched for further studies. Two sets of inclusion criteria were used, minimal (any study of adults undergoing in-hospital cardiopulmonary resuscitation) and strict (included only patients from general ward and intensive care units, and adequately defined cardiopulmonary arrest and resuscitation). Each study was independently reviewed and abstracted in a nonblinded fashion by two reviewers. The data abstracted were compared, and any discrepancies were resolved by consensus discussion. For the subset of studies meeting the strict criteria, the overall rate of immediate survival was 40.7% and the rate of survival to discharge was 13.4%. The following variables were associated with failure to survive to discharge: sepsis on the day prior to resuscitation (odds ratio [OR] 31.3; 95% confidence interval [CI] 1.9, 515), metastatic cancer (OR 3.9; 95% CI 1.2, 12. 6), dementia (OR 3.1; 95% CI 1.1, 8.8), African-American race (OR 2. 8; 95% CI 1.4, 5.6), serum creatinine level at a cutpoint of 1.5 mg/dL (OR 2.2; 95% CI 1.2, 3.8), cancer (OR 1.9; 95% CI 1.2, 3.0), coronary artery disease (OR 0.55; 95% CI 0.4, 0.8), and location of resuscitation in the intensive care unit (OR 0.51; 95% CI 0.4, 0.8).
Conclusions: When talking with patients, physicians can describe the overall likelihood of surviving discharge as 1 in 8 for patients who undergo cardiopulmonary resuscitation and 1 in 3 for patients who survive cardiopulmonary resuscitation.
Figures
References
-
- Murphy DJ. Do-not-resuscitate orders: time for reappraisal in long-term care institutions. JAMA. 1988;260:2098–101. - PubMed
-
- Ruark JE, Raffin TA Stanford University Medical Center Committee on Ethics. Initiating and withdrawing life support: principles and practice in adult medicine. N Engl J Med. 1988;318:25–30. - PubMed
-
- Jonsson PV, McNamee M, Campion EW. The ‘do-not-resuscitate’ order. Arch Intern Med. 1988;148:2373–5. - PubMed
-
- Tomlinson T, Brody H. Ethics and communications in do-not-resuscitate orders. N Engl J Med. 1988;318:43–6. - PubMed
-
- Ebell MH. Practical guidelines for do-not-resuscitate orders. Am Fam Physician. 1994;50:1293–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical