

Aspirin for primary prevention of cardiovascular events
- PMID: 9844080
- PMCID: PMC1497039
- DOI: 10.1046/j.1525-1497.1998.00246.x
Aspirin for primary prevention of cardiovascular events
Abstract
Objective: The use of aspirin for primary prevention of cardiovascular events in the general population is controversial. The purpose of this study was to create a versatile model to evaluate the effects of aspirin in the primary prevention of cardiovascular events in patients with different risk profiles.
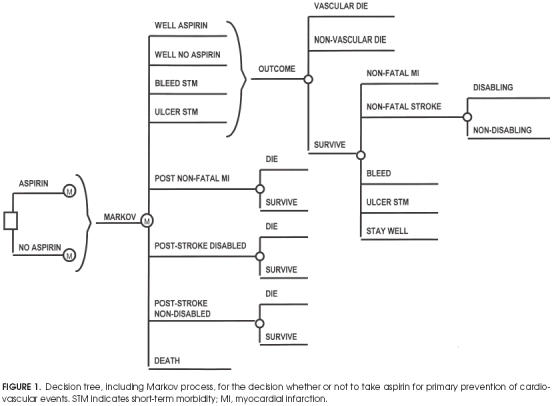
Design: A Markov decision-analytic model evaluated the expected length and quality of life for the cohort's next 10 years as measured by quality-adjusted survival for the options of taking or not taking aspirin.
Setting: Hypothetical model of patients in a primary care setting.
Patients: Several cohorts of patients with a range of risk profiles typically seen in a primary care setting were considered. Risk factors considered included gender, age, cholesterol levels, systolic blood pressure, smoking status, diabetes, and presence of left ventricular hypertrophy. The cohorts were followed for 10 years. Outcomes were myocardial infarction, stroke, gastrointestinal bleed, ulcer, and death.
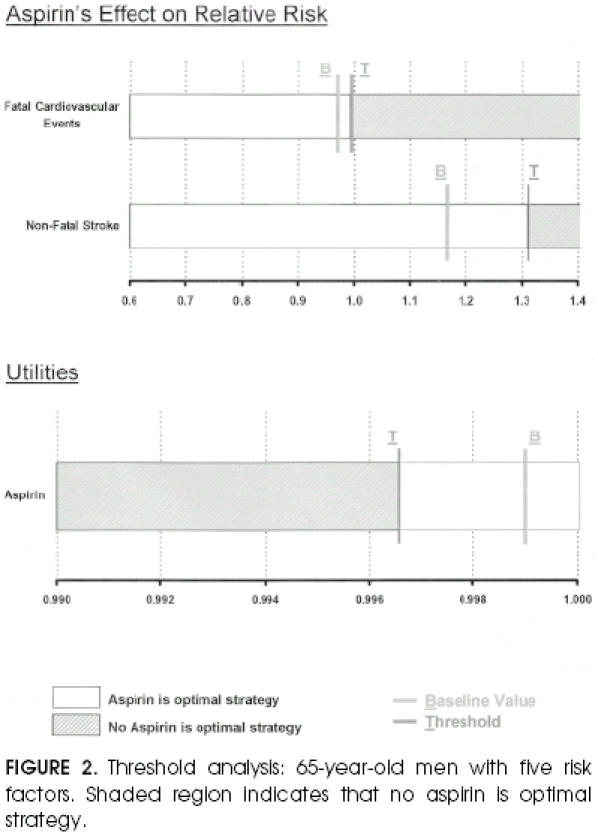
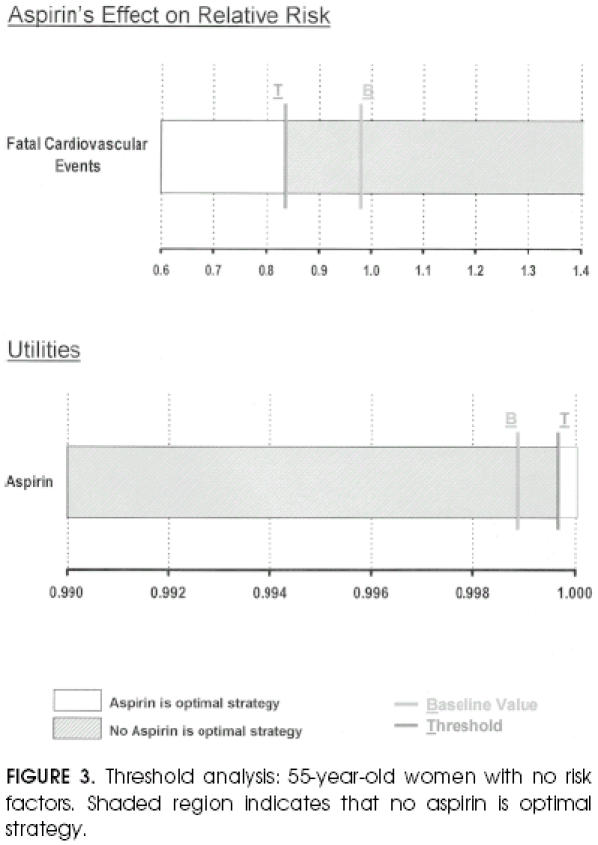
Main results: For the cases considered, the effects of aspirin varied according to the cohort's risk profile. By taking aspirin, the lowest-risk cohort would be the most harmed with a loss of 1.8 quality-adjusted life days by taking aspirin; the highest risk cohort would achieve the most benefit with a gain of 11.3 quality-adjusted life days. Results without quality adjustment favored taking aspirin in all the cohorts, with a gain of 0.73 to 8.04 days. The decision was extremely sensitive to variations in the utility of taking aspirin and to aspirin's effects on cardiovascular mortality. The model was robust to other probability and utility changes within reasonable parameters.
Conclusions: The decision of whether to take aspirin as primary prevention for cardiovascular events depends on patient risk. It is a harmful intervention for patients with no risk factors, and it is beneficial in moderate and high-risk patients. The benefits of aspirin in this population are comparable to those of other widely accepted preventive strategies. It is especially dependent on the patient's risk profile, patient preferences for the adverse effects of aspirin, and on the level of beneficial effects of aspirin on cardiovascular-related mortality.
Figures
References
-
- Guide to Clinical Preventive Services. 2nd. Baltimore, Md:: Williams and Wilkins; 1996. United States Preventive Task Force.
-
- Patrono C. Aspirin as an antiplatelet drug. N Engl J Med. 1994;330:1287–94. - PubMed
-
- The Medical Research Council's General Practice Research Framework. Thrombosis prevention trial: randomised trial of low-intensity oral anticoagulation with warfarin and low-dose aspirin in the primary prevention of ischemic heart disease in men at increased risk. Lancet. 1998;351:233–41. - PubMed
-
- Sonnenberg FA, Beck JR. Markov models in medical decision making: a practical guide. Med Decis Making. 1993;13:322–38. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical