

Rapid identification of nine microorganisms causing acute respiratory tract infections by single-tube multiplex reverse transcription-PCR: feasibility study
- PMID: 9854054
- PMCID: PMC84151
- DOI: 10.1128/JCM.37.1.1-7.1999
Rapid identification of nine microorganisms causing acute respiratory tract infections by single-tube multiplex reverse transcription-PCR: feasibility study
Abstract
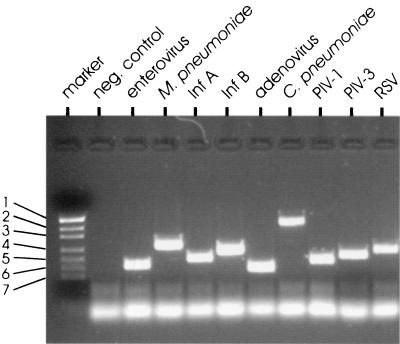
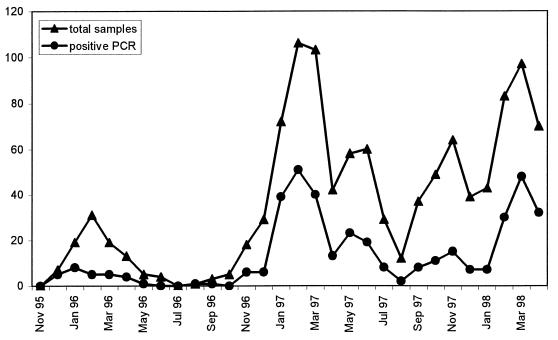
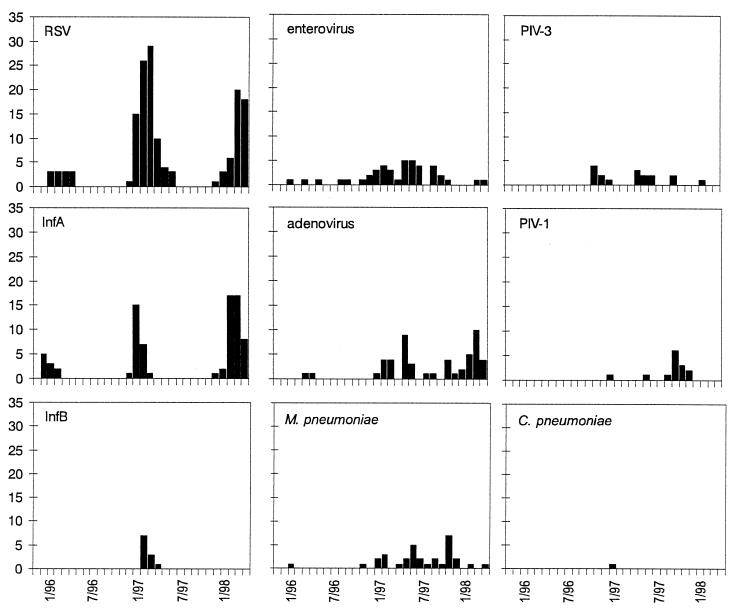
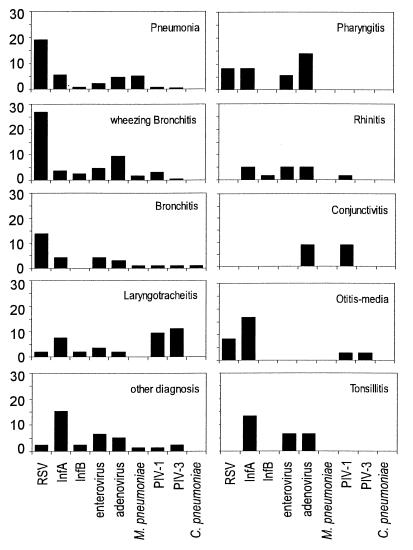
Acute respiratory tract infections (ARIs) are leading causes of morbidity and, in developing countries, mortality in children. A multiplex reverse transcription-PCR (RT-PCR) assay was developed to allow in one test the detection of nine different microorganisms (enterovirus, influenza A and B viruses, respiratory syncytial virus [RSV], parainfluenzaviruses type 1 and type 3, adenovirus, Mycoplasma pneumoniae, and Chlamydia pneumoniae) that do not usually colonize the respiratory tracts of humans but, if present, must be assumed to be the cause of respiratory disease. Clinical samples from 1,118 children admitted to the Department of Pediatrics because of an ARI between November 1995 and April 1998 were used for a first clinical evaluation. Detection of one of the microorganisms included in the assay was achieved for 395 of 1,118 (35%) clinical samples, of which 37.5% were RSV, 20% were influenza A virus, 12.9% were adenovirus, 10.6% were enterovirus, 8.1% were M. pneumoniae, 4.3% were parainfluenzavirus type 3, 3.5% were parainfluenzavirus type 1, 2.8% were influenza B virus, and 0.2% were C. pneumoniae. Seasonal variations in the rates of detection of the different organisms were observed, as was expected from the literature. The levels of concordance with the data obtained by commercially available enzyme immunoassays were 95% for RSV and 98% for influenza A. The results show that the multiplex RT-PCR-enzyme-linked immunosorbent assay is a useful and rapid diagnostic tool for the management of children with ARI. Studies of the overall benefit of this method with regard to the use of antibiotics, the use of diagnostic procedures including additional microbiological tests, and hospitalization rate and duration are warranted.
Figures
References
-
- Adcock P M, Stout G G, Hauck M A, Marshall G S. Effect of rapid viral diagnosis on the management of children hospitalized with lower respiratory tract infection. J Pediatr Infect Dis. 1997;16:842–846. - PubMed
-
- Bartlett J G, Mundy L M. Community-acquired pneumonia. N Engl J Med. 1995;333:1618–1624. - PubMed
-
- Dixon, R. E. 1985. Economic costs of respiratory infections in the United States. Am. J. Med. 78(Suppl. 6B):45–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
