

Transabdominal bowel sonography for the detection of intestinal complications in Crohn's disease
- PMID: 9862836
- PMCID: PMC1760075
- DOI: 10.1136/gut.44.1.112
Transabdominal bowel sonography for the detection of intestinal complications in Crohn's disease
Abstract
Background: The course of Crohn's disease is characterised by the occurrence of intestinal complications such as strictures, intra-abdominal fistulas, or abscesses. Standard diagnostic procedures may fail to show these complications, in particular fistulas.
Aims: To test the value of transabdominal bowel sonography (T) for the detection of intestinal complications in Crohn's disease.
Methods: T was prospectively performed in 213 patients with Crohn's disease in a university based inflammatory bowel disease referral centre. Thirty three underwent resective bowel surgery and were included in this study. The accuracy of T to detect strictures, intra-abdominal fistulas, or abscesses was compared with surgical and pathological findings.
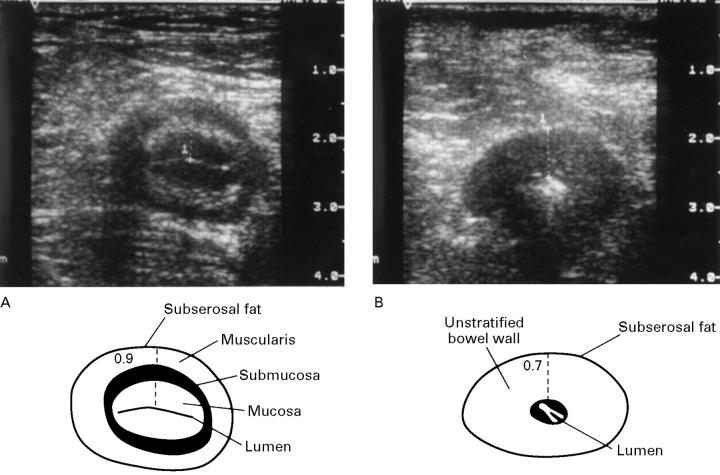
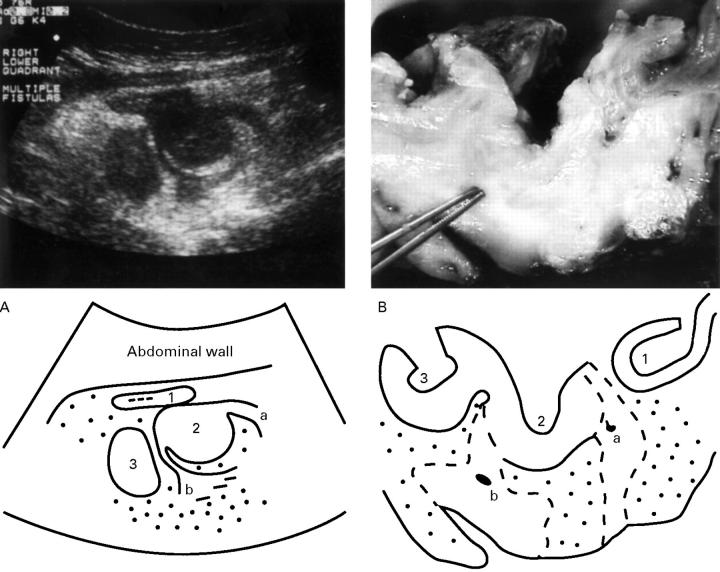
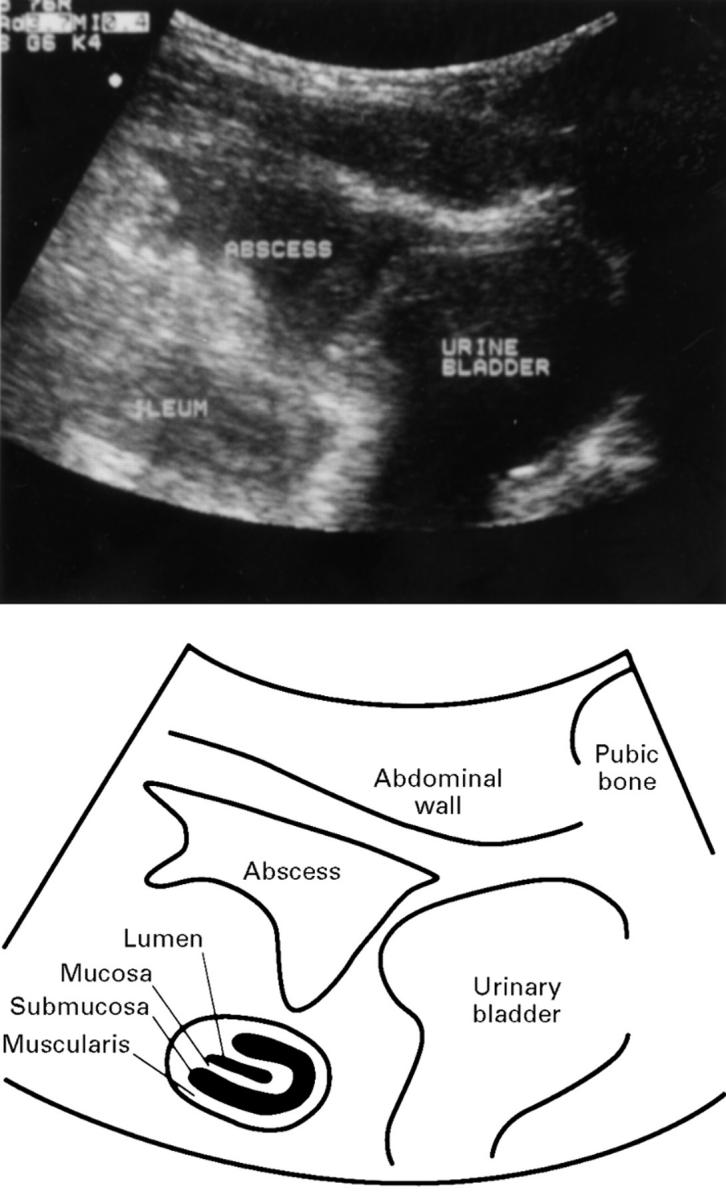
Results: T was able to identify strictures in 22/22 patients and to exclude it in 10/11 patients (100% sensitivity, 91% specificity). Fistulas were correctly identified in 20/23 patients and excluded in 9/10 patients (87% sensitivity, 90% specificity). Intra-abdominal abscesses were correctly detected in 9/9 patients and excluded in 22/24 patients (100% sensitivity, 92% specificity).
Conclusions: In experienced hands T is an accurate method for the detection of intestinal complications in Crohn's disease. T is thus recommended as a primary investigative method for evaluation of severe Crohn's disease.
Figures
Comment in
-
Transabdominal bowel sonography in Crohn's disease.Gut. 1999 Jan;44(1):6-7. doi: 10.1136/gut.44.1.6. Gut. 1999. PMID: 9862816 Free PMC article. No abstract available.
-
Ultrasonographic findings in Crohn's disease.Gut. 2000 Feb;46(2):293. doi: 10.1136/gut.46.2.293. Gut. 2000. PMID: 10712078 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical