

Prognostic factors in patients with endocrine tumours of the duodenopancreatic area
- PMID: 9863490
- PMCID: PMC1727238
- DOI: 10.1136/gut.43.3.422
Prognostic factors in patients with endocrine tumours of the duodenopancreatic area
Abstract
Background: The development of endocrine tumours of the duodenopancreatic area (ETDP) is thought to be slow, but their natural history is not well known. The aim of this study was to determine the factors that influence survival of patients with ETDP.
Patients/methods: Eighty two patients with ETDP (44 non-functioning tumours, 23 gastrinomas, seven calcitonin-secreting tumours, four glucagonomas, three insulinomas, one somatostatinoma) followed from October 1991 to June 1997 were included in the study. The following factors were investigated: primary tumour size, hormonal clinical syndrome, liver metastases, lymph node metastases, extranodular/extrahepatic metastases, progression of liver metastases, local invasion, complete resection of the primary tumour, and degree of tumoral differentiation. The prognostic significance of these factors was investigated by uni- and multi-variate analysis.
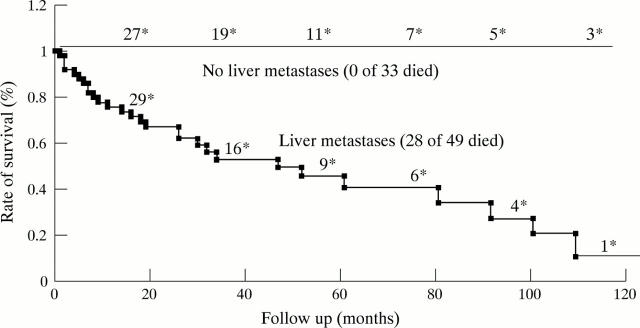
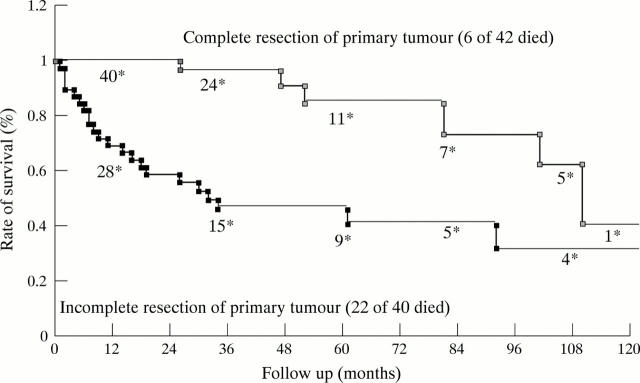
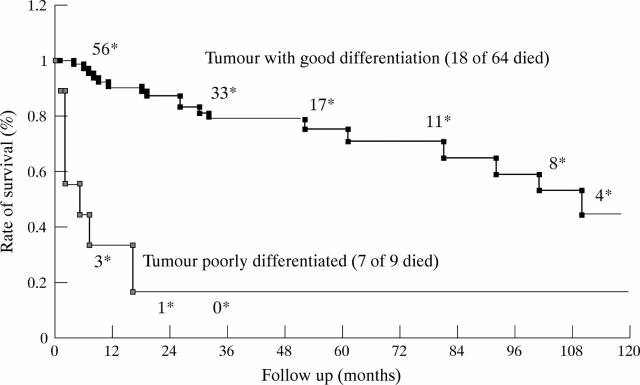
Results: Twenty eight patients (34%) died within a median of 17 months (range 1-110) from diagnosis. Liver metastases (p = 0.001), lymph node metastases (p = 0.001), progression of liver metastases (p < 0.00001), lack of complete resection of the primary tumour (p = 0.001), extranodular/extrahepatic metastases (p = 0.001), local invasion (p = 0.001), primary tumour size > or = 3 cm (p = 0.001), non-functioning tumours (p = 0.02), and poor tumoral differentiation (p = 0.006) were associated with an unfavourable outcome by univariate analysis. Multivariate analysis identified only liver metastases (risk ratio (RR) = 8.3; p < 0.0001), poor tumoral cell differentiation (RR = 8.1; p = 0.0001), and lack of complete resection of the primary tumour (RR = 4.8; p = 0.0007) as independent risk factors. Five year survival rates were 40 and 100% in patients with and without liver metastases, 85 and 42% in patients with and without complete resection of primary tumour, and 17 and 71% in patients with poor and good tumour cell differentiation respectively.
Conclusion: Liver metastases are a major prognostic factor in patients with ETDP. Progression of liver metastases is also an important factor which must be taken into account when deciding on the therapeutic approach. The only other independent prognostic factors are tumoral cell differentiation and complete resection of the primary tumour.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical