

Efficacy of trovafloxacin in treatment of experimental staphylococcal or streptococcal endocarditis
- PMID: 9869569
- PMCID: PMC89024
- DOI: 10.1128/AAC.43.1.77
Efficacy of trovafloxacin in treatment of experimental staphylococcal or streptococcal endocarditis
Abstract
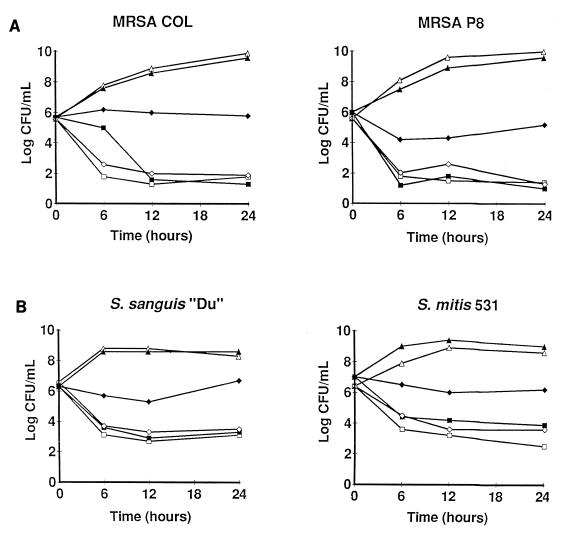
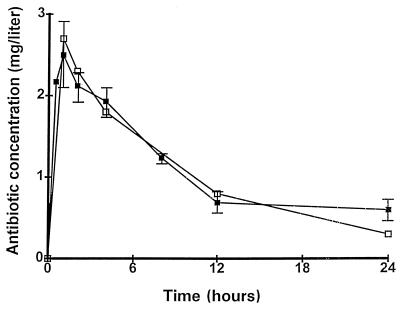
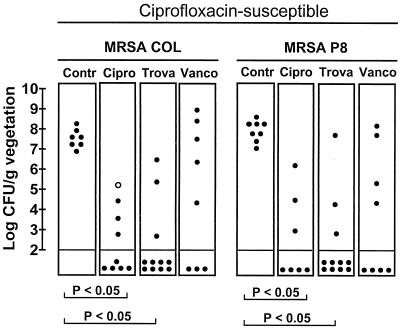
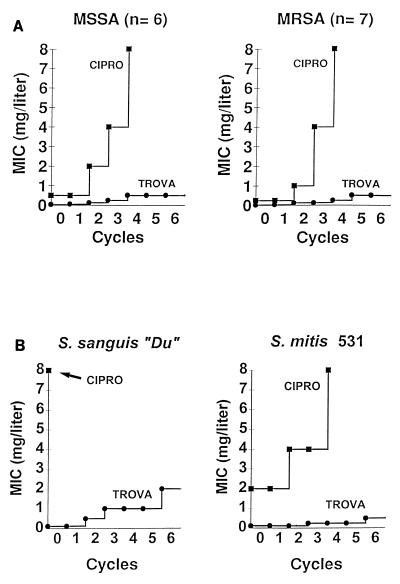
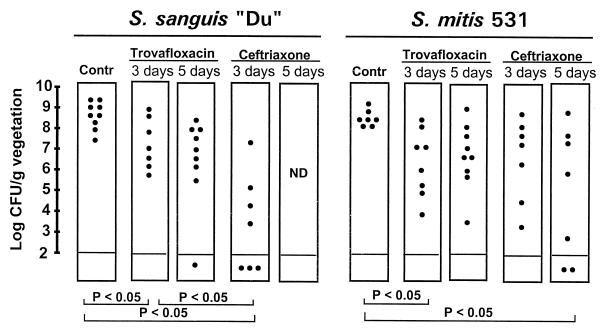
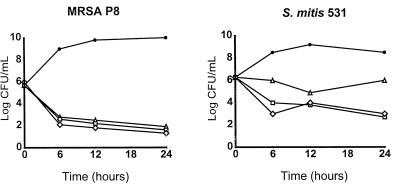
The efficacy of trovafloxacin against Staphylococcus aureus and viridans group streptococci was investigated in vitro and in an experimental model of endocarditis. The MICs at which trovafloxacin and ciprofloxacin inhibited 90% of clinical isolates of such bacteria (MIC90s) were (i) 0.03 and 2 mg/liter, respectively, for 30 ciprofloxacin-susceptible S. aureus isolates, (ii) 32 and 128 mg/liter, respectively, for 20 ciprofloxacin-resistant S. aureus isolates, and (iii) 0.25 and 8 mg/liter, respectively, for 28 viridans group streptococci. Rats with aortic vegetations were infected with either of two ciprofloxacin-susceptible but methicillin-resistant S. aureus strains (strains COL and P8), one penicillin-susceptible Streptococcus sanguis strain, or one penicillin-resistant Streptococcus mitis strain. Rats were treated for 3 or 5 days with doses that resulted in kinetics that simulated those achieved in humans with trovafloxacin (200 mg orally once a day), ciprofloxacin (750 mg orally twice a day), vancomycin (1 g intravenously twice a day), or ceftriaxone (2 g intravenously once a day). Against the staphylococci, the activities of both trovafloxacin and ciprofloxacin were equivalent to that of vancomycin, and treatment of endocarditis with these drugs was successful (P < 0.05). However, ciprofloxacin selected for resistant derivatives in vitro and in vivo, whereas trovafloxacin was 10 to 100 times less prone than ciprofloxacin to select for resistance in vitro and did not select for resistance in vivo. Against the two streptococcal isolates, trovafloxacin significantly (P < 0.05) decreased bacterial counts in the vegetations but was less effective than the control drug, ceftriaxone. Thus, a simulated oral dose of trovafloxacin (200 mg per day) was effective against ciprofloxacin-susceptible staphylococci and was less likely than ciprofloxacin to select for resistance. The simulated oral dose of trovafloxacin also had some activity against streptococcal endocarditis, but optimal treatment of infections caused by such organisms might require higher doses of the drug.
Figures
References
-
- Barry A L, Brown S D, Fuchs P C. In vitro-selection of quinolone-resistant staphylococcal mutants by single exposure to ciprofloxacin or trovafloxacin (CP-99,219) J Antimicrob Chemother. 1996;38:324–327. - PubMed
-
- Blatter M, Entenza J, Moreillon P, Glauser M P. Program and abstracts of the 33rd Interscience Conference on Antimicrobial Agents and Chemotherapy. Washington, D.C: American Society for Microbiology; 1993. Parenteral sparfloxacin compared to vancomycin in the treatment of experimental endocarditis due to methicillin-resistant Staphylococcus aureus, abstr. 150; p. 147.
-
- Blum M D, Graham D J, McCloskey C A. Temafloxacin syndrome: review of 95 cases. Clin Infect Dis. 1993;18:946–950. - PubMed
-
- Borner K, Höffken G, Lode H, Koeppe P, Prinzing C, Glatzel P, Wiley R, Olschewski P, Sievers B, Reinitz D. Pharmacokinetics of ciprofloxacin in healthy volunteers after oral and intravenous administration. Eur J Clin Microbiol. 1986;5:179–186. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
