

Review
Chronic rejection. A general overview of histopathology and pathophysiology with emphasis on liver, heart and intestinal allografts
Affiliations
- PMID: 9869851
- PMCID: PMC3235804
Item in Clipboard
Review
Chronic rejection. A general overview of histopathology and pathophysiology with emphasis on liver, heart and intestinal allografts
Ann Transplant.
1997.
No abstract available
Figures
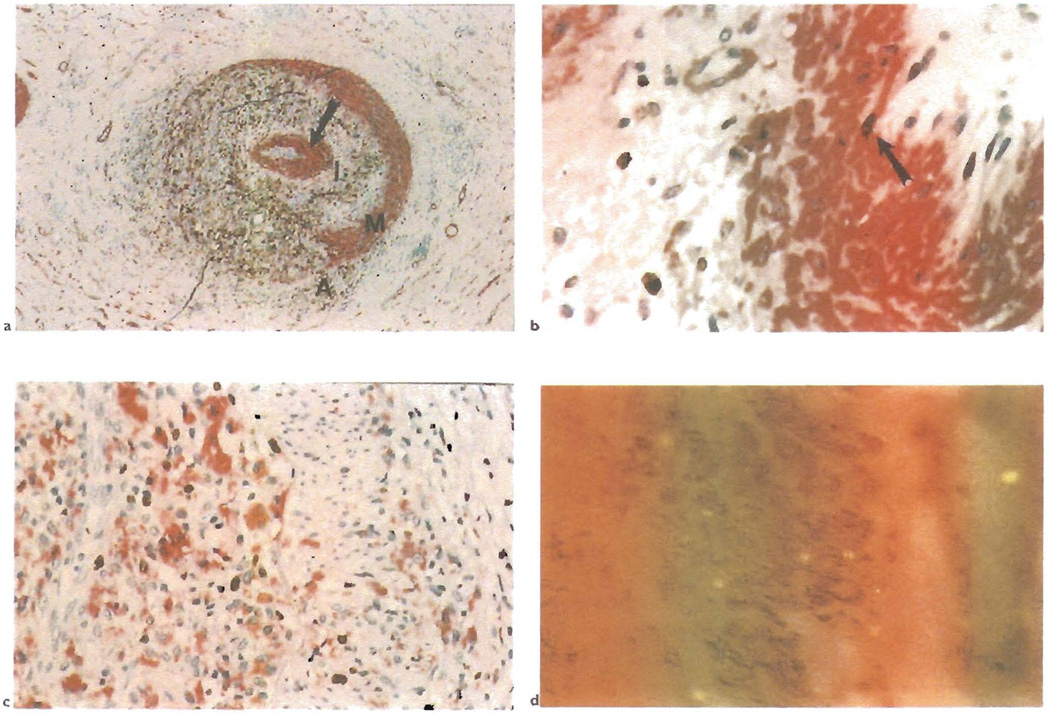
a) This section shows a hepatic artery branch in the hilum of a liver allograft. It is stained with a double immunolabeling procedure for smooth muscle actin(red) and macrophages(CD68: brown). Note the severe lumenal narrowing because of obliterative arteriopathy and destruction of the media along one half of its circumference(A = adventitia: M = media: I = intima). Note also the concentric ring of myofibroblasts(arrow) that separates the deep intimal macrophages from the endothelium, which is intact and uninflammed. Extension of the macrophages from the adventitia through to the deep intima suggests that some of the arterial inflammation may begin in the adventitia and may contribute to the development of OA without directly involving the intima. b) A higher magnification of the subendothelial ring of myofibroblasts shows them to be micotically active{arrow: double staining for smooth muscle actin (red) and proliferating cells. Ki-67 (brown)}. c) The ring of deep intimal inflammatory cells is also mitotically active{double staining for macrophages (CD68: red) and proliferating cells, Ki-67 (brown)}. d) Double labeling for smooth muscle cells(actin; brown) and male cells (Y chromosome in situ hybridization, yellow dot) shows that the intimal myofibroblasts in the female recipient of a male liver are of donor origin.
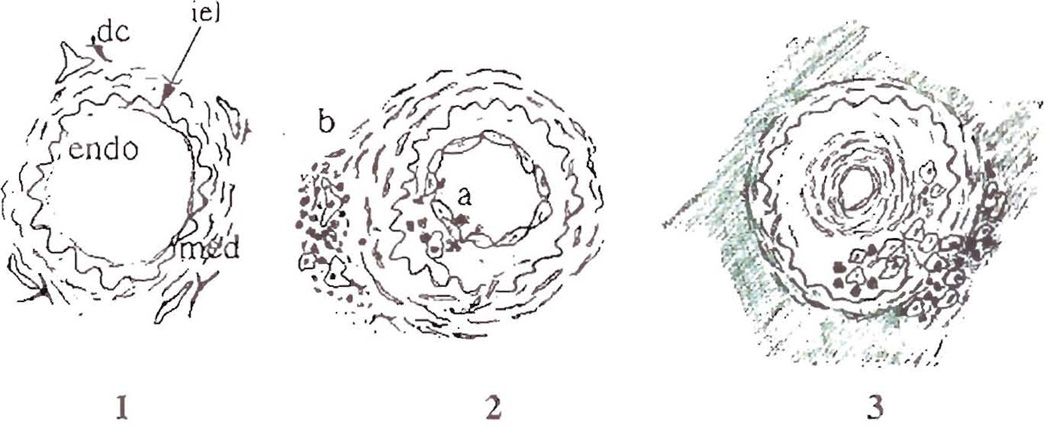
Schematic of the sequential steps in the development of obliterative arteriopathy, which is the common feature of chronic rejection in all solid organ allografts. A normal artery is shown in frame 1, illustrating the important anatomic features including the endothelial lining (endo), which is flattened and inactive-appearing, the internal elastic lamina (iel), the media (med) and the dendritic cells(dc) located near draining lymphatics in the adventitia of arteries. Frame 2 shows early arterial changes during acute rejection and two distinct, but not mutually exclusive pathways of arterial injury. In severe acute rejection(a) the endothelium and intima can be directly injured by antibodies/complement and/or inflammatory cells, which leads to an intimal repair response and myofibroblast proliferation. However, arterial damage can also occur in less severe rejection episodes, illustrated by pathway (b). Inflammatory cells accumulate near adventitial donor dendritic cells and draining lymphatics. This causes edema of the media and intima with damage of individual medial myocytes, and indirect injury of the endothelium. Endothelial hypertrophy and activation occur with both insults and the arterial repair response is triggered. Frame 3 illustrates some of the latter charges in the development of OA. A concentric ring of myofibroblasts develops immediately subjacent to the endothelium, which returns to a more quiescent appearance. The media also becomes thinner, presumably as a result or migration of myocytes to the intima and/or compensatory arterial dilatation. The macrophages and lymphocytes now accumulate in the deep intima and focally stream through the disrupted media. This results in a connection between the intimal inflammatory cells and the cuff of macrophages and lymphocytes in the adventitia. The arrangement suggests that adventitial to intimal trafficking of immune cells is an important entry route. It occurs at a time when fibrosis is developing in the adventitia around affected anteries and in the interstitium.
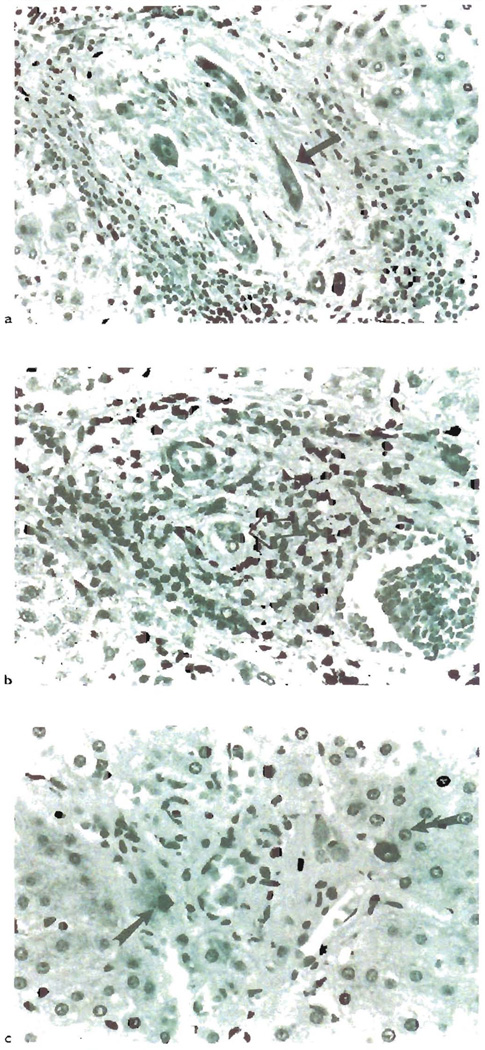
a) This section some of the most characteristic changes associated with the earlier phases of chronic liver allograft rejection. Note the “atrophic” appearance of the biliary epithelium(arrow). There is uneven spacing of the epithelial cells, eosinophilic transformation of the cytoplasm and local pyknosis. b) Interstingly, even though these duccal cells are “atrophic” appearing, they can show an increased proliferation rate, as determined by Ki-67 staining(arrow): c) Eventually, the small bile ducts are completely destroyed in chronic liver allograft rejection. Cytokeratin staining can be used to help identify the ducts, but it is usually not needed [288]. Whether these few periportal cytokeratin-19+ cells in this chronically rejected liver(arrows), represent progenitor cells capable of regenerating the ducts, is worthy of further study(see text).
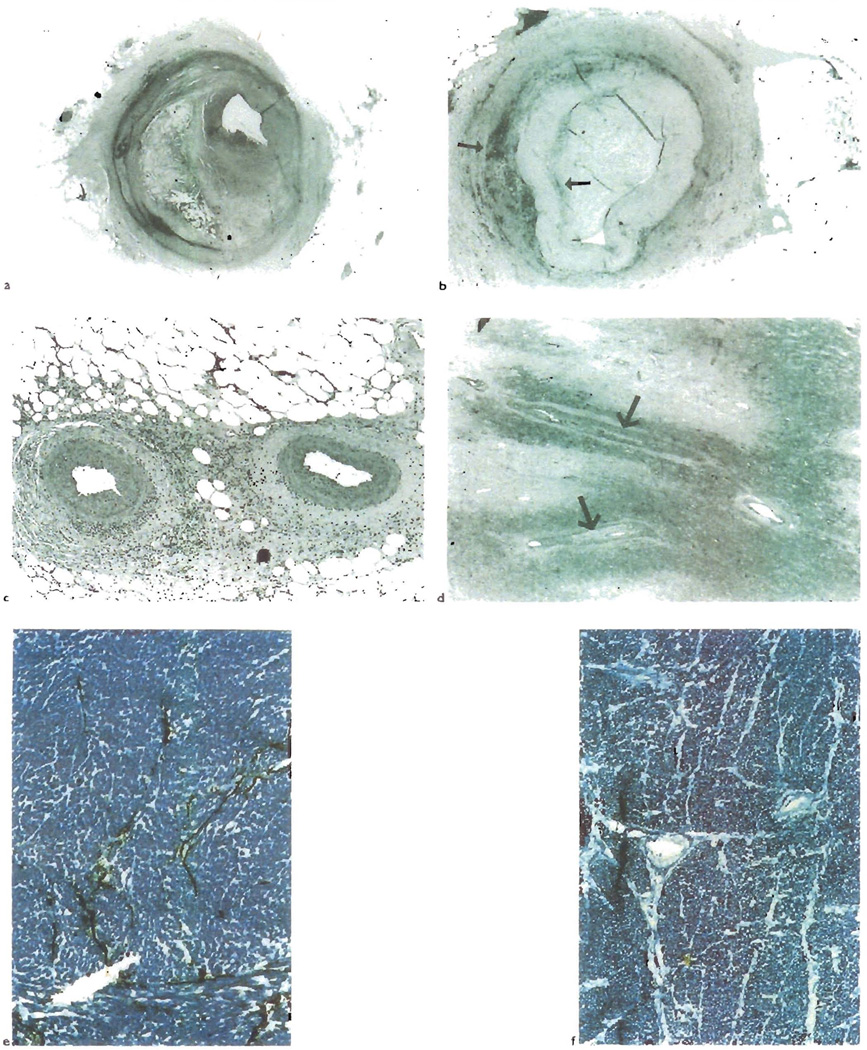
a) Atherosclerotic lesions involving the epicardial coronary arteries are frequently eccentric and show cholesterol clefts, as is seen in this lesion from a cardiac allograft. b) However, OA lesion can also have an eccentric distribution as shown here. Note the cuff of adventitial and deep intimal macrophages (arrows, CD68), similar to that seen in Figure 1 from a liver allograft. c) In contrast to acherosclerosis, OA often involves the distal branches of the epicardial coronary arteries and d) even those smaller intra-myocardial branches (arrows). There is also destruction of the lymphatic microvasculature of the heart in CR (e and f) Compare the lymphatic channels (black, histochemical stain for 5 nucleortidase) traversing the fibrous septae with arteries in a normal heart(e), with the lack of staining seen in cardiac allograft with CR(f)
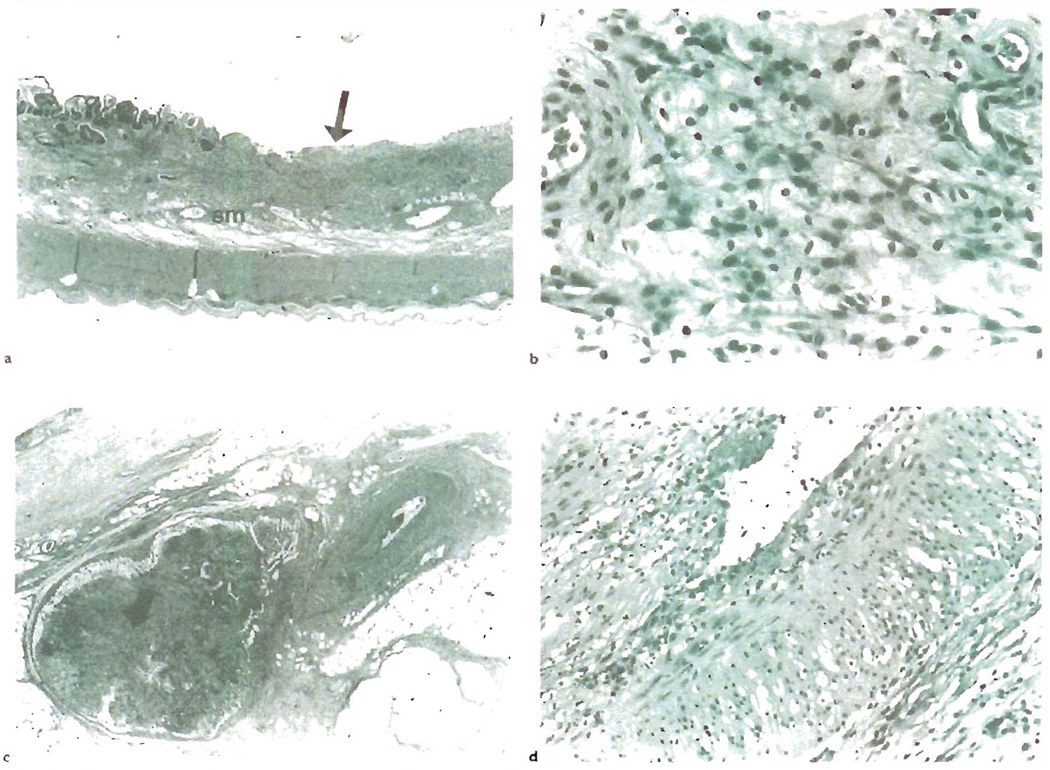
a) CR of human small bowel allograft shows focal, non-healing ulcers(arrow), as shown here, and thickening and fibrosis of the submucosa(sm). b) A higher magnification of the submucosa reveals abundant foam cell deposition, similar to that seen in the arterial intima of blood vessels with OA. c) Like other allografts, the arteries affected by OA are not commonly sampled in biopsies. This section shows a mesenteric artery with OA near a mesenteric lymph node with lymphold depletion and fibrosis(arrow). d) A higher magnification shows mild lymphocytic intimal inflammation, intimal foam cell deposition and endothelial cell hypertrophy. Note also the marked medial vacuolization, which is due to foam cell infiltration between myocytes and intercellular edema.
References
-
- Billingham ME. Pathology of graft vascular disease after heart and heart-lung transplantation and its relationship to obliterative bronchiolitis. [Review][17 refs] Transplant Proc. 1995;27(3):2013–2016. - PubMed
-
- Cramer DV. Cardiac Graft Atherosclerosis. In: Paul LC, Solez K, editors. Organ Transplantation: long-term results. New York, NY: Marcel Dekker; 1992. pp. 173–195.
-
- Balk AHMM, Weintar W. Chronic Heart Graft Rejection in the Clinical Setting. In: Paul LC, Solez K, editors. Organ Transplantation: long-term results. New York, NY: Marcel Dekker; 1992. pp. 187–195.
-
- Berry GJ, Rizeq MN, Weiss LM, Billingham ME. Graft coronary disease in pediatric heart and combined heart-lung transplant recipients: a study of fifteen cases. Journal of Heart & Lung Transplantation. 1993;12(6 Pt 2):S309–S319. - PubMed
-
- Radley-Smith RC, Burke M, Pomerance A, Yacoub MH. Graft vessell disease and obliterative bronchiolitis after heart/lung transplantation in children. Transplant Proceed. 1995;27:2017–2018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical