

Endoscopic management of adnexal masses
Abstract
Background: The laparoscopic management of suspicious adnexal masses and early ovarian malignancies is discussed with the aim of maintaining accepted oncologic treatment principles. Comparative survival data of patients with gynecological malignancies managed by laparoscopy or laparotomy are still very scarce and the survival of cancer patients must not be compromised by new techniques. It is time to closely analyze laparoscopy and determine if it has a positive impact on the diagnosis and treatment of ovarian malignancies. In this paper we will address the following points: 1) Which ovarian cysts can be surgically treated by laparoscopy (pelviscopy)? 2) Is staging laparoscopy an accepted technique? 3) Is laparoscopy, as a second-look procedure, of benefit? 4) Is laparoscopic staging, together with histologic tissue sampling, adequate surgical technique in inoperable ovarian cancer with ascites and peritoneal carcinomatosis? 5) Does endoscopic biopsy of ovarian cancer stage Ia change the destiny of a patient into ovarian cancer Ic?
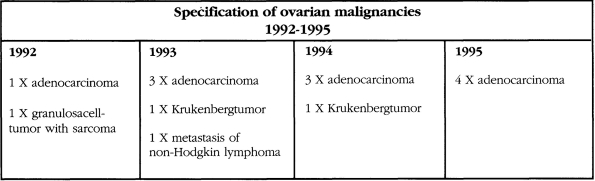
Data base: The above questions are analyzed based on our experience with the laparoscopic treatment of 1,225 patients with ovarian cysts and 165 ovarian cancer patients stage I to IV treated immediately by laparotomy during the years 1992-1995.
Conclusions: Ovarian cystic tumors with no signs of malignancy can be dealt with by laparoscopic means with the option of immediate conversion to laparotomy or within one week if an ovarian malignancy is diagnosed. Today sampling laparoscopic lymphadenectomy of both pelvic and para-aortic is feasible and adequate. On a curative level, the number of lymph nodes to be resected has yet to be determined. The adnexa can be extracted from the abdominal cavity with bag extraction without the danger of spillage. The uterus can be removed transvaginally with laparoscopic assisted vaginal hysterectomy (LAVH). We must be cautious to advocate laparoscopy for ovarian cancer. However, it is an excellent tool when used as a staging procedure. A careful preoperative screening of the patient and an exact definition of existing cysts with imaging techniques allows us to frequently apply laparoscopic surgery for ovarian cysts, leaving only readily detectable cancer cases for laparotomy. Many gynecological oncologists employing staging and second-look procedures for ovarian cancer agree that initiating a case with laparoscopy may preclude laparotomy for many patients. Tumor propagation by performing a biopsy in FIGO stage Ia ovarian cancer patients does not occur if the patient receives adequate radical surgical treatment within one week. According to the reports of Sevelda et al. and Dembo et al., the degree of differentiation and the existence of ascites are more relevant to decreasing the five-year survival rate of patients with ovarian cancer stage I than the rupture of capsule or penetration of the tumor. A dependency on the first two parameters was found in these two large statistical studies. As the question of endoscopic operations for adnexal mass is predominantly put for the sanitation of small ovarian tumors (ovarian tumors with solid particles in the cysts can be put into the section of primary laparotomies) there remains a wide field of indications for the laparoscopic treatment of adnexal mass and ovarian cysts with benign indications. For many young patients with non-malignant ovarian lesions such as endometriosis, benign cysts, benign cystic proliferations and fibromas, a laparotomy can be avoided and these lesions treated by laparoscopy.
Figures
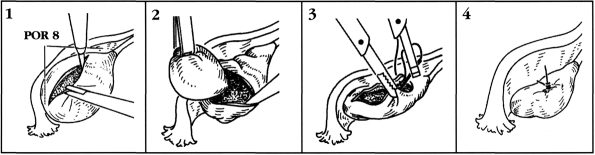
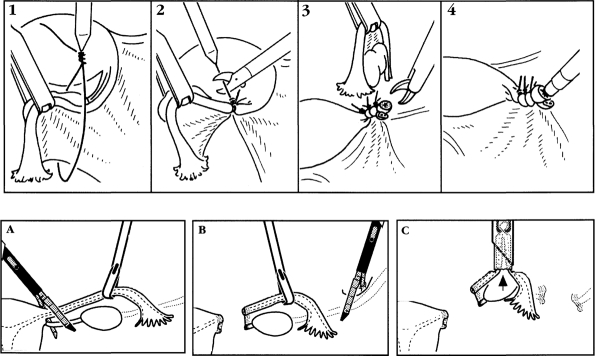
1. Capsular incision
2. Cyst resection
3. Ovarian suture
4. Final aspect after endoscopic ovarian cyst resection
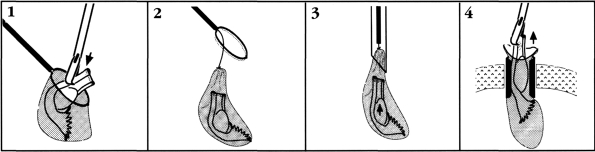
1. Positioning of adnexa into an endobag
2. Closing the bag by pulling the string
3. Insertion of bag into the trocar
4. Bag extraction
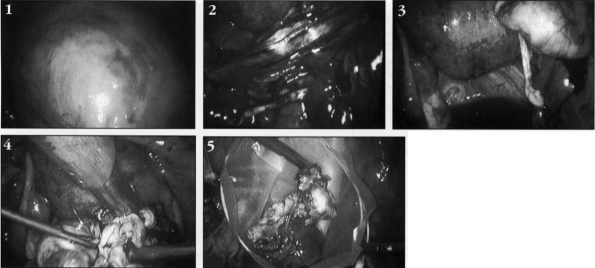
1. Ovarian cyst to the right side
2. Cyst resection
3. Cyst inspection
4. Ovarian suture
5. Endobag extraction
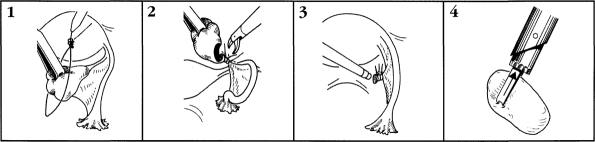
1. Positioning of the frist Roeder loop
2. After placement of 3 loops ovarian resection
3. Endocoagulation of the ovarian stump
4. Ovarian morcellation using 15 or 20 mm trocars
1. Placement of first loop
2. Cutting the loop
3. After positioning of 3 loops adnexal resection
4. Endocoagulation of the stump
A. Adnexal resection using a stapling device at the ovarian ligamnet
B. Dissection of infundihulo pelvic ligament
C. Adnexal resection
Similar articles
-
Unexpected ovarian malignancy found after laparoscopic surgery in patients with adnexal masses--a single institutional experience.Nagoya J Med Sci. 2014 Feb;76(1-2):83-90. Nagoya J Med Sci. 2014. PMID: 25129994 Free PMC article.
-
Role of laparoscopy in the diagnosis and treatment of adnexal masses.Chin Med J (Engl). 2006 Feb 5;119(3):202-6. Chin Med J (Engl). 2006. PMID: 16537005
-
Management of adnexal masses: role and risk of laparoscopy.Semin Surg Oncol. 2000 Jul-Aug;19(1):28-35. doi: 10.1002/1098-2388(200007/08)19:1<28::aid-ssu5>3.0.co;2-c. Semin Surg Oncol. 2000. PMID: 10883021
-
Laparoscopic management of adnexal masses: a gold standard?Curr Opin Obstet Gynecol. 2002 Aug;14(4):423-8. doi: 10.1097/00001703-200208000-00010. Curr Opin Obstet Gynecol. 2002. PMID: 12151833 Review.
-
Diagnosis and management of organic ovarian cysts: indications and procedures for laparoscopy.Hum Reprod Update. 1996 Sep-Oct;2(5):435-46. doi: 10.1093/humupd/2.5.435. Hum Reprod Update. 1996. PMID: 15717442 Review.
Cited by
-
Laparoscopic management of adnexal masses.JSLS. 2001 Apr-Jun;5(2):143-51. JSLS. 2001. PMID: 11394427 Free PMC article.
-
Laparoscopic versus open resection for sigmoid diverticulitis.Cochrane Database Syst Rev. 2017 Nov 25;11(11):CD009277. doi: 10.1002/14651858.CD009277.pub2. Cochrane Database Syst Rev. 2017. PMID: 29178125 Free PMC article.
-
Laparoscopic Cystectomy In-a-Bag of an Intact Cyst: Is It Feasible and Spillage-Free After All?Minim Invasive Surg. 2016;2016:8640871. doi: 10.1155/2016/8640871. Epub 2016 Mar 23. Minim Invasive Surg. 2016. PMID: 27099793 Free PMC article.
-
Laparoscopic removal of a large ovarian mass utilizing planned trocar puncture.JSLS. 2012 Jan-Mar;16(1):148-50. doi: 10.4293/108680812X13291597716465. JSLS. 2012. PMID: 22906344 Free PMC article.
-
Criteria for Laparoscopic Advanced Surgery in Semi-Equipped Setup (CLASS): Feasibility Study Based on Institutional Experience.Indian J Surg. 2014 Feb;76(1):31-7. doi: 10.1007/s12262-012-0597-2. Epub 2012 Jun 17. Indian J Surg. 2014. PMID: 24799781 Free PMC article.
References
-
- Semm K. Operative Manual for Endoscopic Abdominal Surgery. Chicago, IL, London, UK: Yearbook Medical Publishers, 1984:339–340
-
- Bagley CM, Young RC, Schein PS, Chabner BA, DeVita VT. Ovarian cancer metastatic to diaphragm frequently underdiagnosed at laparotomy, a preliminary report. Am J Obstet Gynecol 1973;116:397–400 - PubMed
-
- Ozóls RF, Fisher RI, Anderson T. Peritoneoscopy in the management of ovarian carcinoma. Am J Obstet Gynecol. 1981;l40:6ll–623 - PubMed
-
- Berek JS, Griffiths CT, Levanthal JM. Laparoscopy for second-look evaluation in ovarian carcinoma. Obstet Gynecol. 1992;58:192–198 - PubMed
-
- Mettler L, Caesar G, Neunzling S, Semm K. Stellenwert der endoskopischen Ovar-Chirurgie - kritische Analyse von 626 pelviskopisch operierten Ovarialzysten an der Universitatsfrauenklinik Kiel 190-1991. Geburtsbilfe Frauenbeilkunde. 1993;53:253–257 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials