

Using an outcomes-based approach to identify candidates for risk stratification after exercise treadmill testing
- PMID: 9893084
- PMCID: PMC1496439
- DOI: 10.1046/j.1525-1497.1999.00273.x
Using an outcomes-based approach to identify candidates for risk stratification after exercise treadmill testing
Abstract
Objective: To develop a hierarchical approach to cardiac risk stratification after treadmill testing.
Patients: Clinical and treadmill test data were used to identify a patient population that may be candidates for further risk stratification with stress tomographic myocardial perfusion imaging. A prospective series of 3, 620 medically treated patients (42% female, mean age 63 years) with a 2.5% mortality was identified (follow-up 2.5 +/- SD 1.5 years).
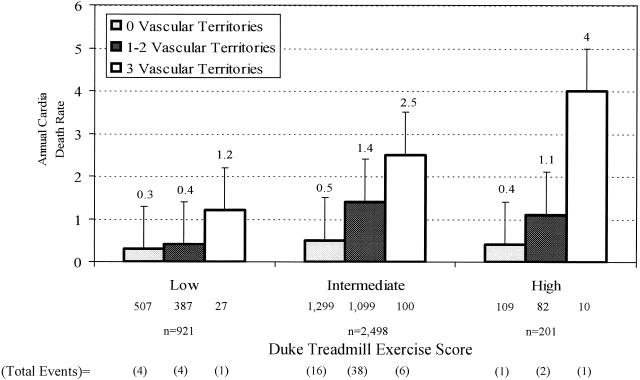
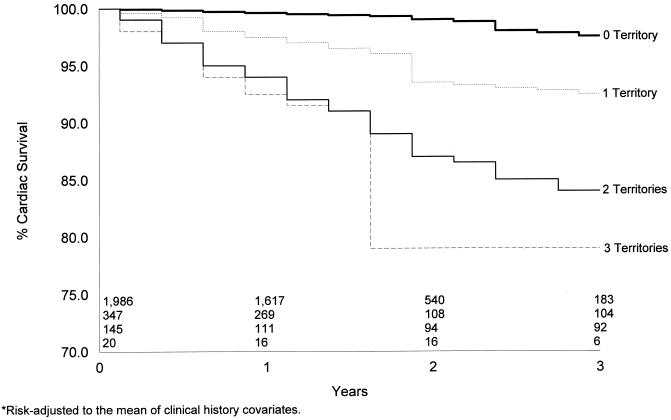
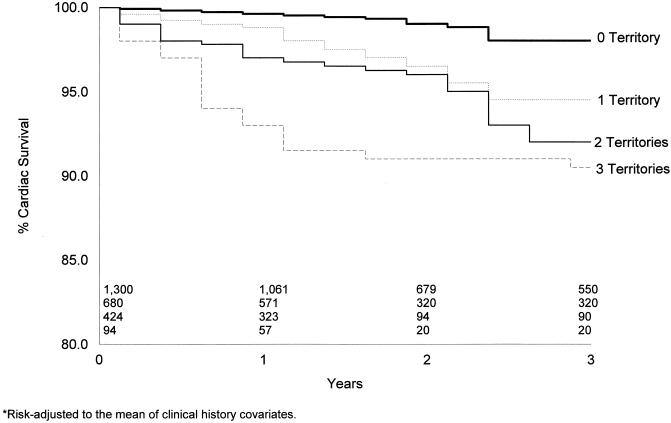
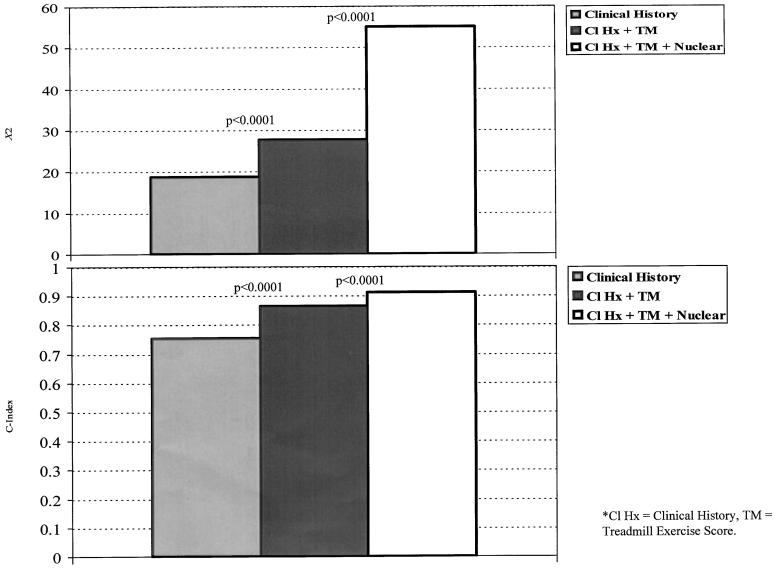
Measurements and main results: A Cox proportional hazards model was used to estimate a patient's likelihood of cardiac death. Kaplan-Meier survival curves were used to estimate time to cardiac death by nuclear test results. Annual rates of cardiac death were 0. 4% (n = 921), 1% (n = 2,498), and 1% (n = 201) for patients with low, intermediate, and high Duke treadmill scores (DTS). For patients with an intermediate DTS, multivariate estimators of cardiac death included the number of ischemic vascular territories (relative risk per defect 1.4, p =.01), the number of infarcted vascular territories (relative risk per defect 2.4, p =.00001), and the DTS (relative risk per unit 0.97, p =.00001), following adjustment for a patient's pretest risk of coronary disease. For patients with an intermediate DTS, the presence of no, one or two, and three vascular territories with defects was associated with annual rates of cardiac death of 0.5%, 1.4%, and 2.5%, respectively (p <.0001). Kaplan-Meier survival curves exhibited a statistically worsening survival for patients with defects by 1 year after treadmill exercise.
Conclusions: For symptomatic patients with an intermediate treadmill test score, the exercise myocardial perfusion scan may be used to stratify their risk of cardiac death over 3 years of follow-up. Patient management may be efficiently guided by further outcome assessment, with an exercise nuclear scan for patients whose treadmill test score is intermediate.
Figures
Comment in
-
Exercise testing to predict outcome in patients with angina.J Gen Intern Med. 1999 Jan;14(1):63-5. doi: 10.1046/j.1525-1497.1999.00283.x. J Gen Intern Med. 1999. PMID: 9893094 Free PMC article. No abstract available.
References
-
- Mark DB, Shaw L, Harrell FE, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med. 1991;325:849–53. - PubMed
-
- Mark DB, Hlatky MA, Harrell FE, Jr, Lee KL, Califf RM, Pryor DB. Exercise treadmill score for predicting prognosis in coronary artery disease. Ann Intern Med. 1987;106:793–800. - PubMed
-
- Mark DB, Hlatky MA, Lee KL, Harrell FE, Jr, Califf RM, Pryor DB. Localizing coronary artery obstructions with the exercise treadmill test. Ann Intern Med. 1987;106:53–5. - PubMed
-
- Hlatky MA, Pryor DB, Harrell FE, Jr, Califf RM, Mark DB, Rosati RA. Factors affecting sensitivity and specificity of exercise electrocardiography. Am J Med. 1984;77:64–71. - PubMed
-
- Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med. 1993;118:689–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources