

Increased gastric PCO2 during exercise is indicative of gastric ischaemia: a tonometric study
- PMID: 9895373
- PMCID: PMC1727400
- DOI: 10.1136/gut.44.2.163
Increased gastric PCO2 during exercise is indicative of gastric ischaemia: a tonometric study
Abstract
Background: Diagnosis of gastric ischaemia is difficult and angiography is an invasive procedure. Angiographic findings may not correlate with clinical importance.
Aims: To investigate whether tonometric measurement of intragastric PCO2 during exercise can be used to detect clinically important gastric ischaemia.
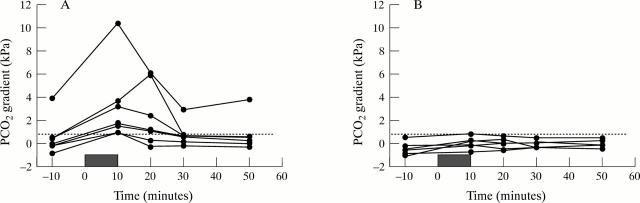
Methods: Fourteen patients with unexplained abdominal pain or weight loss were studied. Splanchnic angiography served as the gold standard. Three patients were studied again after a revascularisation procedure. Gastric PCO2 was measured from a nasogastric tonometer, with 10 minute dwell times, and after acid suppression. Gastric and capillary PCO2 were measured before, during, and after submaximal exercise of 10 minutes duration.
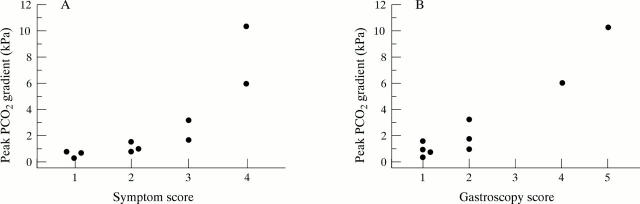
Results: Seven patients had normal angiograms; seven had more than 50% stenosis in the coeliac (n=7) or superior mesenteric artery (n=4). Normal subjects showed no changes in tonometry. In patients with stenoses, the median intragastric PCO2 (PiCO2) at rest was 5.2 kPa (range 4.8-11.2) and rose to 6.4 kPa (range 5.7-15.7) at peak exercise; the median intragastric blood PCO2 gradient increased from 0.0 kPa (range -0.8 to 5.9) to 1.7 kPa (range 0.9 to 10.3; p<0.01). Only two subjects had abnormal tonometry at rest; all had supernormal values at peak exercise. The PCO2 gradient correlated with clinical and gastroscopic severity; in patients reexamined after revascularisation (n=3), exercise tonometry returned to normal.
Conclusion: Gastric tonometry during exercise is a promising non-invasive tool for diagnosing and grading gastrointestinal ischaemia and evaluating the results of revascularisation surgery for symptomatic gastric ischaemia.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources