

Is there a rationale for rationing chronic dialysis? A hospital based cohort study of factors affecting survival and morbidity
- PMID: 9915728
- PMCID: PMC27700
- DOI: 10.1136/bmj.318.7178.217
Is there a rationale for rationing chronic dialysis? A hospital based cohort study of factors affecting survival and morbidity
Abstract
Objectives: To determine factors influencing survival and need for hospitalisation in patients needing dialysis, and to define the potential basis for rationing access to renal replacement therapy.
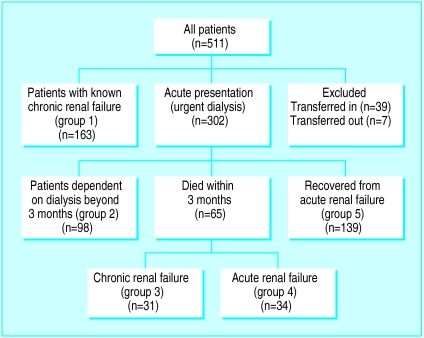
Design: Hospital based cohort study of all patients starting dialysis over a 4 year recruitment period (follow up 15-63 months). Groups were defined on the basis of age, comorbidity, functional status, and whether dialysis initiation was planned or unplanned.
Setting: Renal unit in a district general hospital, which acts as the main renal referral centre for four other such hospitals and serves a population of about 1.15 million people.
Subjects: 292 patients, mean age 61.3 years (18-92 years, SD 15.8), of whom 193 (66%) were male, and 59 (20%) were patients with diabetes. Dialysis initiation was planned in 163 (56%) patients and unplanned in 129 (44%).
Main outcome measures: Overall survival, 1 year survival, and hospitalisation rate.
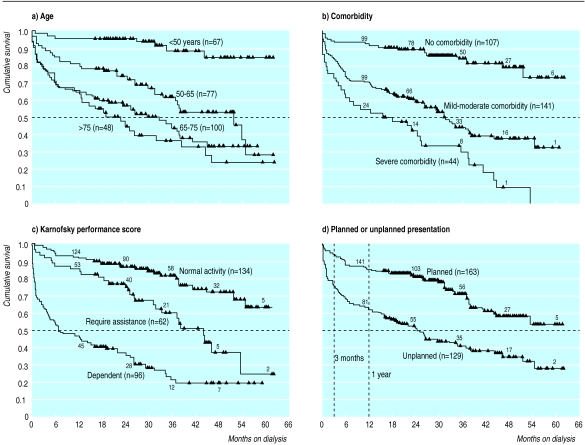
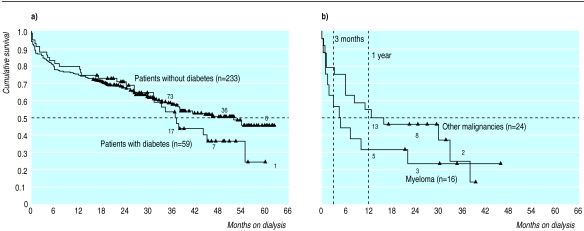
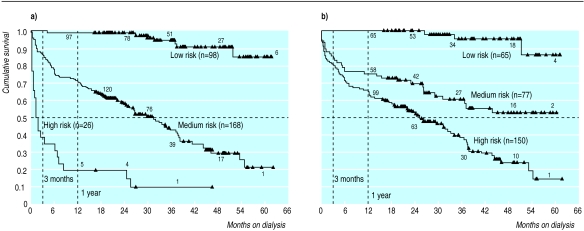
Results: Factors affecting survival in the Cox's proportional hazard model were Karnofsky performance score at presentation (hazard ratio 0.979, 95% confidence interval 0.972 to 0. 986), comorbidity severity score (1.240, 1.131 to 1.340), age (1.036, 1.018 to 1.054), and myeloma (2.15, 1.140 to 4.042). The Karnofsky performance score used 3 months before presentation was significant (0.970, 0.956 to 0.981), as was unplanned presentation in this model (1.796, 1.233 to 2.617). Using these factors, a high risk group of 26 patients was defined, with 19.2% 1 year survival. Denying dialysis to this group would save 3.2% of the total cost of the chronic programme but would sacrifice five long term survivors. Less rigorous definition of the high risk group would save more money but lose more long term survivors.
Conclusions: Severity of comorbid conditions and functional capacity are more important than age in predicting survival and morbidity of patients on dialysis. Late referral for dialysis affects survival adversely. Denial of dialysis to patients in an extremely high risk group, defined by a new stratification based on logistic regression, would be of debatable benefit.
Figures
Comment in
-
Is there a rationale for rationing chronic dialysis? Study's objectives were not achieved.BMJ. 1999 Jun 12;318(7198):1619; author reply 1620. BMJ. 1999. PMID: 10428556 No abstract available.
-
Is there a rationale for rationing chronic dialysis? Question is difficult to address on basis of retrospective studies.BMJ. 1999 Jun 12;318(7198):1619-20. BMJ. 1999. PMID: 10428557 No abstract available.
References
-
- Davies R, Roderick P. Predicting the future demand for renal replacement therapy in England using simulation modelling. Nephrol Dial Transplant. 1997;12:2512–2516. - PubMed
-
- Hull AR. The legislative and regulatory process in the end-stage renal disease (ESRD) program, 1973 through 1997. Semin Nephrol. 1997;17:160–169. - PubMed
-
- Friedman EA. Rationing of uremia therapy. Artificial Organs. 1992;16:90–97. - PubMed
-
- Mendelssohn DC, Kua BT, Singer PA. Referral for dialysis in Ontario. Arch Intern Med. 1995;155:2473–2478. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical