

Emmetropisation, axial length, and corneal topography in teenagers with Down's syndrome
- PMID: 9924374
- PMCID: PMC1722688
- DOI: 10.1136/bjo.82.7.793
Emmetropisation, axial length, and corneal topography in teenagers with Down's syndrome
Abstract
Aim: To study the refractive status and corneal topography in Down's syndrome.
Method: A matched cohort subgroup of 50 individuals with Down's syndrome in the Manchester area aged 15-22 years was studied by refraction, corneal topography, A-scan biometry, slit lamp examination, and orthoptic examination.
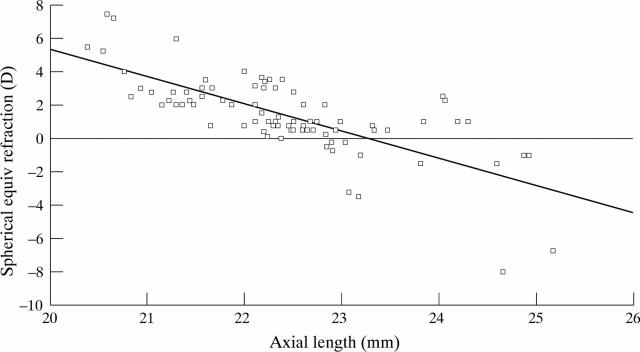
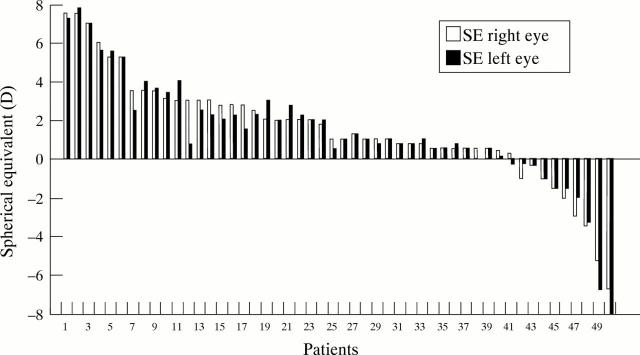
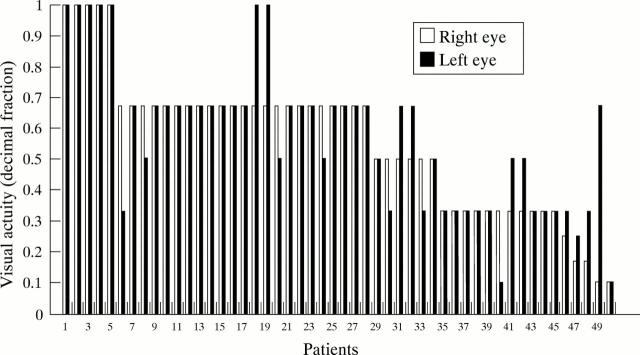
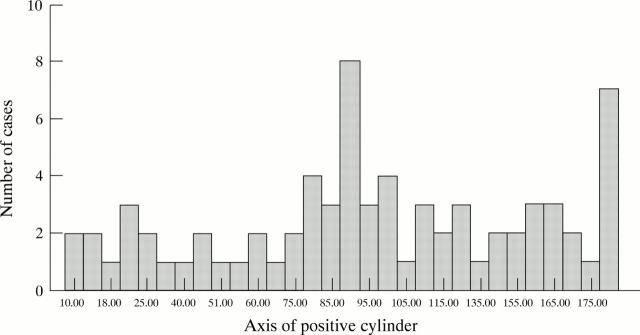
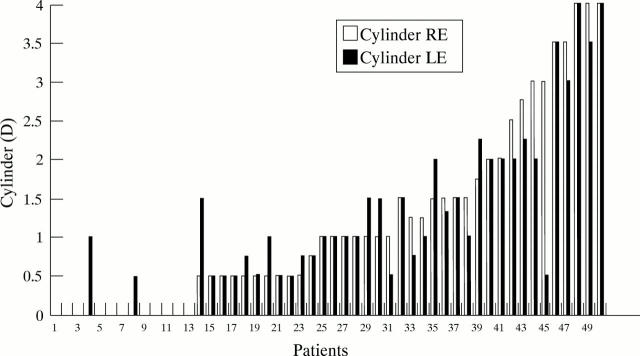
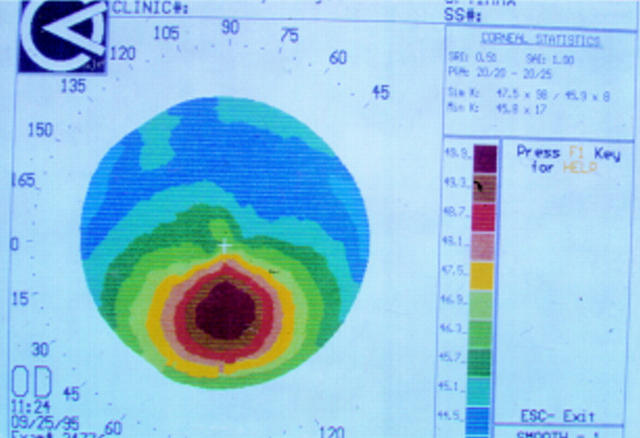
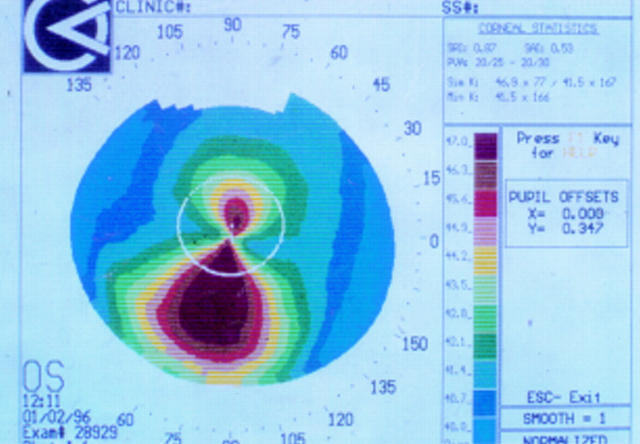
Results: (1) A linear relation was found between axial length and spherical equivalent refraction. There was no statistical relation between keratometry and the axial length. (2) 80% of the group had a hyperopic refraction (mean +2.46 D, range +0.5 to +7.5 D); 18% were myopic (mean -2.75 D, range -0.5 to -8.0 D); and 2% were emmetropic (within plus or minus 0.5 D of zero). The overall mean spherical equivalent refraction was +1.43 (SD 2.86) D. 63% of eyes could see 6/12 or better and 66% of the individuals had a binocular vision of 6/12 or better. (3) Corneal topography was generally of a regular "bow tie" pattern, but there was a high incidence of oblique cylinders. Mean cylinder strength was 1.14 (1.15) D. (4) The prevalence of overt keratoconus was 2%. 6% had corneal topography with inferior steepening which may be a preclinical keratoconic process.
Conclusions: In this cohort of late teenagers with Down's syndrome, emmetropisation has failed to occur in most individuals. In a similar aged group of non-disabled individuals one would expect about 83% emmetropic (plus or minus 0.25 D), 13% myopic, and 4% hyperopic. The wide spread of oblique cylinders and the small proportion of with the rule astigmatism is probably related to this failure of emmetropisation. The prevalence of 2% keratoconus in Down's syndrome compares with that found by other authors of between 5.5 and 15%. The 6% with inferior steepening on topography will be followed up over the next few years to see if there is any development of clinical keratoconus. Hence we will see if corneal topography is useful as a screening tool for preclinical keratoconus in this high risk group.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous