

IgG subclass reactivity to human cardiac myosin in cardiomyopathy patients is indicative of a Th1-like autoimmune disease
- PMID: 9933448
- PMCID: PMC1905170
- DOI: 10.1046/j.1365-2249.1999.00807.x
IgG subclass reactivity to human cardiac myosin in cardiomyopathy patients is indicative of a Th1-like autoimmune disease
Abstract
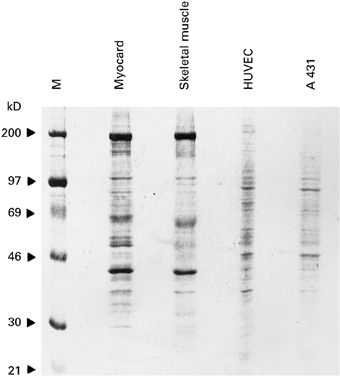
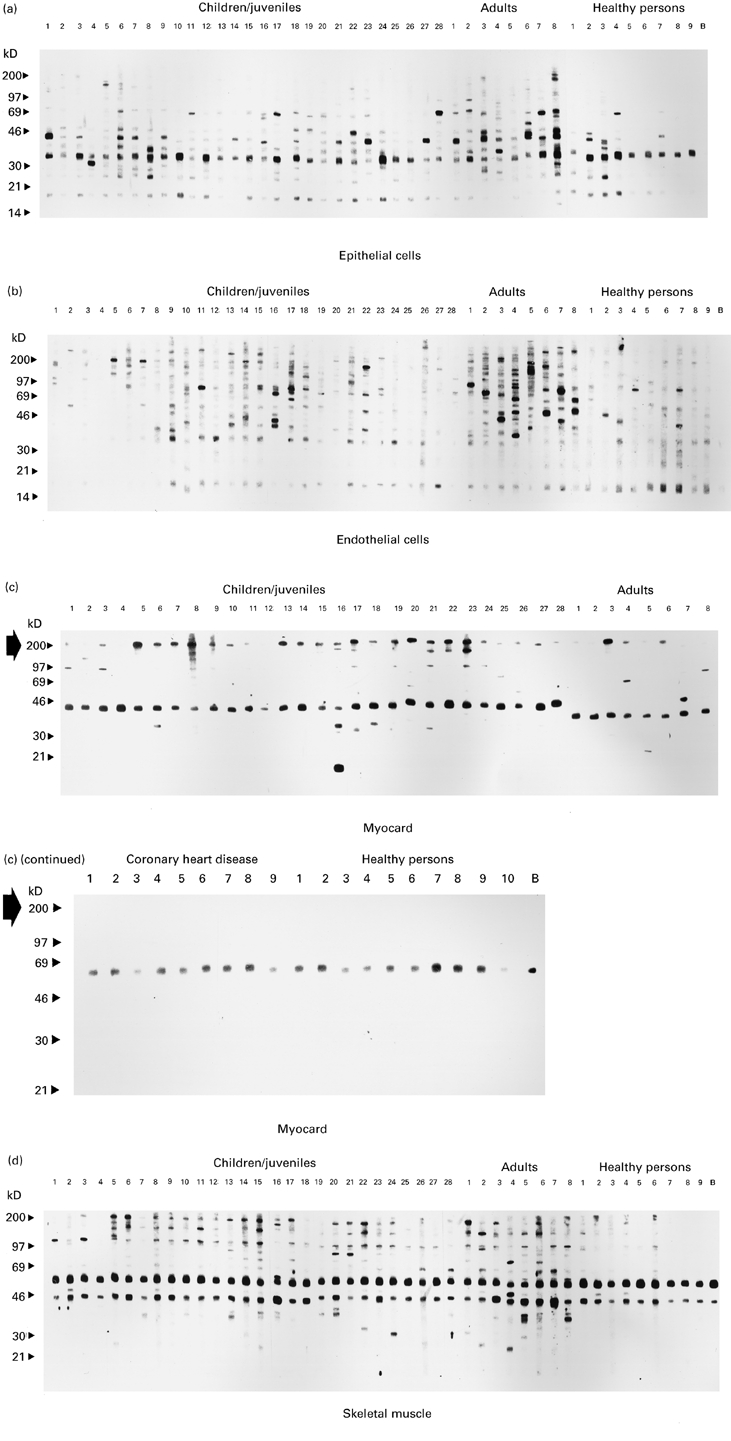
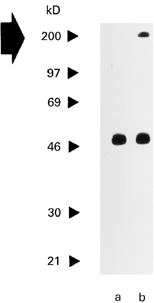
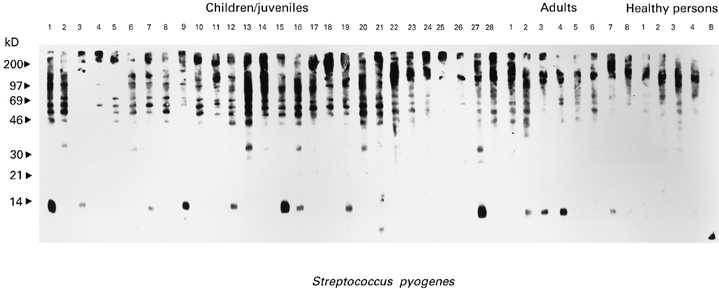
Studies performed in mice together with the demonstration of increased levels of heart-specific autoantibodies, cytokines and cytokine receptors in sera from cardiomyopathy (CMP) patients argued for a pathogenic role of autoimmune mechanisms in CMP. This study was designed to analyse the presence of IgG anti-heart antibodies in sera from patients suffering from hypertrophic and dilatative forms of CMP as well as from patients with ischaemic heart disease and healthy individuals. Patients' sera were analysed for IgG reactivity to Western-blotted extracts prepared from human epithelial and endothelial cells, heart and skeletal muscle specimens as well as from Streptococcus pyogenes. The IgG subclass (IgG1-4) reactivity to purified human cardiac myosin was analysed by ELISA. While sera from CMP patients and healthy individuals displayed comparable IgG reactivity to a variety of human proteins, cardiac myosin represented the prominent antigen detected strongly and preferentially by sera from CMP patients. Pronounced IgG anti-cardiac myosin reactivity was frequently found in sera from patients with dilatative CMP and reduced ventricular function. ELISA analyses revealed a prominent IgG2/IgG3 anti-cardiac myosin reactivity in CMP sera, indicating a preferential Th1-like immune response. Elevated anti-cytomegalovirus, anti-enterovirus IgG titres as well as IgG reactivity to nitrocellulose-blotted S. pyogenes proteins were also frequently observed in the group of CMP patients. If further work can support the hypothesis that autoreactivity to cardiac myosin represents a pathogenic factor in CMP, specific immunomodulation of this Th1- towards a Th2-like immune response may represent a promising therapeutic strategy for CMP.
Figures
References
-
- Hein S, Schaper J. Pathogenesis of dilated cardiomyopathy and heart failure: insights from cell morphology and biology. Curr Opin Cardiol. 1996;11:293–301. - PubMed
-
- Kuhn H, Gietzen F, Beer G, Pethig K. Epidemiology of idiopathic dilated cardiomyopathy. In: Figulla HR, Kandolf R, McManus B, editors. Idiopathic dilated cardiomyopathy: cellular and molecular mechanisms, clinical consequences. Berlin: Springer-Verlag; 1993. pp. 13–25.
-
- Durand JB, Bachinski LL, Bieling LC, et al. Localization of a gene responsible for familial dilated cardiomyopathy to chromosome 1q32. Circulation. 1995;92:3387–9. - PubMed
-
- Tanigawa G, Jarcho JA, Kass S, et al. A molecular basis for familial hypertrophic cardiomyopathy: an α/β cardiac myosin heavy chain hybrid gene. Cell. 1990;62:991–8. - PubMed
-
- Geisterfer-Lowrance AAT, Kass S, Tanigawa G, et al. A molecular basis for familial hypertrophic cardiomyopathy: a β cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999–1006. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
