

Association between lactate-to-albumin ratio and mortality in hepatic failure: a retrospective cohort study
- PMID: 40155840
- PMCID: PMC11951681
- DOI: 10.1186/s12879-025-10783-z
Association between lactate-to-albumin ratio and mortality in hepatic failure: a retrospective cohort study
Abstract
Background: Liver failure has a high mortality rate, and currently, there is no convenient risk predictor. The lactate-to-albumin ratio (LAR) has emerged as a promising predictor in various critical illnesses. However, its potential role in predicting all-cause mortality in patients with liver failure remains unexplored. Therefore, this study aims to investigate the correlation between LAR and all-cause mortality in patients suffering from liver failure.
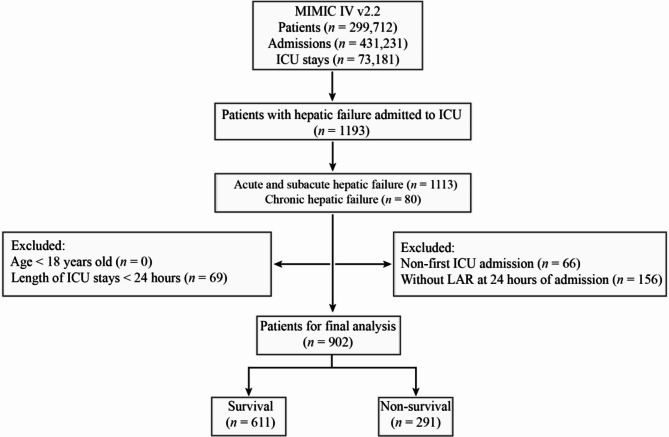
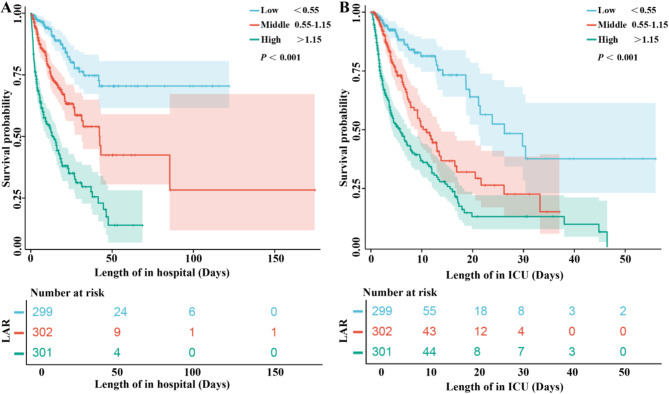
Methods: We retrospectively analyzed data from patients with liver failure who were admitted to the intensive care unit (ICU) between 2008 and 2019, which were gathered from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. LAR was calculated from the ratio obtained from the first measurement taken within 24 h of admission. The optimal LAR threshold was determined using the Youden index. With LAR categorized into low, middle, and high groups based on tertiles, Kaplan - Meier analysis was employed to compare mortality risks among three patient groups. Multivariate Cox proportional hazards regression models were utilized to evaluate the association between LAR and all-cause mortality in hepatic failure patients within hospital admission. Additionally, receiver operating characteristic (ROC) and smoothing curve analysis were used to assess the predictive ability, sensitivity, and specificity of LAR for all-cause mortality in patients with liver failure, and the area under the curve (AUC) was calculated. A smooth curve fitting approach and threshold effect analysis were employed to detect the potentially non-linear relationship between the LAR and the risk of all-cause mortality in patients with hepatic failure. Finally, subgroup analyses were performed to assess the relationship between LAR and prognosis across different types of liver failure.
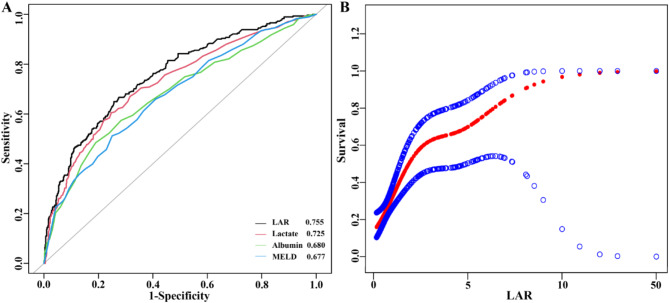
Results: A total of 902 patients with hepatic failure were included in this study. They were divided into survivors group (611 patients) and non-survivors group (291 patients) according to whether they survived during hospitalization, and the mortality rate of patients was 32.26%. The Kaplan-Meier survival curves illustrating patients in hepatic failure with elevated LAR showed a significantly heightened risk of in-hospital mortality (P < 0.001). We identified a non-linear relationship between LAR and the risk of hospital mortality after adjusting for potential confounders and the inflection point of LAR to be 1.33. LAR was shown to be an independent predictor of all-cause mortality within hospitalization in patients with hepatic failure by multivariate COX regression analysis (HR, 1.66; 95% CI, 1.35-2.05; P < 0.0001). The optimal cutoff value for separating the survival and death groups according to ROC was found to be 0.97. The AUC value for LAR was 0.755 (95% CI: 0.721, 0.789), which was higher than that for arterial blood lactate (AUC = 0.725) and serum albumin (AUC = 0.680) alone. It was not inferior even when compared to MELD (AUC = 0.677).
Conclusion: LAR has demonstrated good predictive value for all-cause mortality among liver failure patients in our retrospective study.
Keywords: All-cause mortality; Cohort; Hepatic failure; LAC.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study utilized the MIMIC-IV database, which received approval from the Institutional Review Boards of Beth Israel Deaconess Medical Center in Boston, Massachusetts, and the Massachusetts Institute of Technology. To safeguard patient privacy, all personal data is deidentified, with random codes replacing patient identification. And this was a retrospective analysis, an ethical approval statement and the informed consent was not required for this study in accordance with the national legislation and the institutional requirements. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Abbreviations: All abbreviations used in this study can be found in Supplementary Table 2. Foundation: This work was supported by the Science and Technology Fund Project of Guizhou Health Commission in 2024 (No. gzwkj2024-010), the Guizhou Provincial Science and Technology Projects (QKH JC-ZK [2024]-210; QKH JC-zk[2025]-461), and Cultivation Program for Regional Projects of the National Natural Science Foundation of China (No. gyfynsfc[2024]-19).
Figures
Similar articles
-
Lactate-to-albumin ratio as a potential prognostic predictor in patients with cirrhosis and sepsis: a retrospective cohort study.BMC Infect Dis. 2025 Feb 14;25(1):223. doi: 10.1186/s12879-025-10601-6. BMC Infect Dis. 2025. PMID: 39953385 Free PMC article.
-
Association between lactate-to-albumin ratio and 28-days all-cause mortality in patients with acute pancreatitis: A retrospective analysis of the MIMIC-IV database.Front Immunol. 2022 Dec 14;13:1076121. doi: 10.3389/fimmu.2022.1076121. eCollection 2022. Front Immunol. 2022. PMID: 36591285 Free PMC article.
-
Association between lactate-to-albumin ratio and short-time mortality in patients with acute respiratory distress syndrome.J Clin Anesth. 2024 Dec;99:111632. doi: 10.1016/j.jclinane.2024.111632. Epub 2024 Sep 26. J Clin Anesth. 2024. PMID: 39326299
-
Association Between Lactate-to-Albumin Ratio and 28-Day All-Cause Mortality in Critical Care Patients with COPD: Can Both Arterial and Peripheral Venous Lactate Serve as Predictors?Int J Chron Obstruct Pulmon Dis. 2025 May 11;20:1419-1434. doi: 10.2147/COPD.S503625. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40376192 Free PMC article.
-
Lactate-to-Albumin Ratio (LAR) as a Predictor of All-Cause Mortality in Patients With Myocardial Infarction: A Systematic Review and Meta-Analysis.Cureus. 2025 Apr 13;17(4):e82166. doi: 10.7759/cureus.82166. eCollection 2025 Apr. Cureus. 2025. PMID: 40364881 Free PMC article. Review.
Cited by
-
The role of the Lactate-to-Albumin ratio in predicting ICU admission and mortality in patients with UGIB presenting to the ED: a prospective observational study.BMC Emerg Med. 2025 Jul 1;25(1):99. doi: 10.1186/s12873-025-01261-5. BMC Emerg Med. 2025. PMID: 40596811 Free PMC article.
References
-
- Flamm SL, Yang YX, Singh S, Falck-Ytter YT, Committee AGAICG. American gastroenterological association Institute guidelines for the diagnosis and management of acute liver failure. Gastroenterology. 2017;152(3):644–7. - PubMed
-
- Barosa R, Roque Ramos L, Patita M, Nunes G, Fonseca J. CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with acute on chronic liver failure admitted to the ward. Rev Esp Enferm Dig. 2017;109(6):399–405. - PubMed
-
- Ferrarese A, Bucci M, Zanetto A, Senzolo M, Germani G, Gambato M, Russo FP, Burra P. Prognostic models in end stage liver disease. Best Pract Res Clin Gastroenterol. 2023;67:101866. - PubMed
-
- Duseja A, Choudhary NS, Gupta S, Dhiman RK, Chawla Y. APACHE II score is superior to SOFA, CTP and MELD in predicting the short-term mortality in patients with acute-on-chronic liver failure (ACLF). J Dig Dis. 2013;14(9):484–90. - PubMed
-
- Mishra A, Rustgi V. Prognostic models in acute liver failure. Clin Liver Dis. 2018;22(2):375–88. - PubMed
MeSH terms
Substances
Grants and funding
- gzwkj2024-010/the Science and Technology Fund Project of Guizhou Health Commission in 2024
- QKH JC-ZK [2024]-210/the Guizhou Provincial Science and Technology Projects
- QKH JC-zk[2025]-461/the Guizhou Provincial Science and Technology Projects
- No. gyfynsfc[2024]-19/Cultivation Program for Regional Projects of the National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Miscellaneous
