

Adiponectin and Glucocorticoids Modulate Risk for Preterm Birth: The Healthy Start Study
- PMID: 38980936
- PMCID: PMC12102719
- DOI: 10.1210/clinem/dgae464
Adiponectin and Glucocorticoids Modulate Risk for Preterm Birth: The Healthy Start Study
Abstract
Context: Adiponectin is a potent uterine tocolytic that decreases with gestational age, suggesting it could be a maternal metabolic quiescence factor. Maternal stress can influence preterm birth risk, and adiponectin levels may be stress responsive.
Objective: We characterized associations between adiponectin and glucocorticoids with preterm birth and modeled their predictive utility. We hypothesized maternal plasma adiponectin and cortisol are inversely related and lower adiponectin and higher cortisol associate with preterm birth.
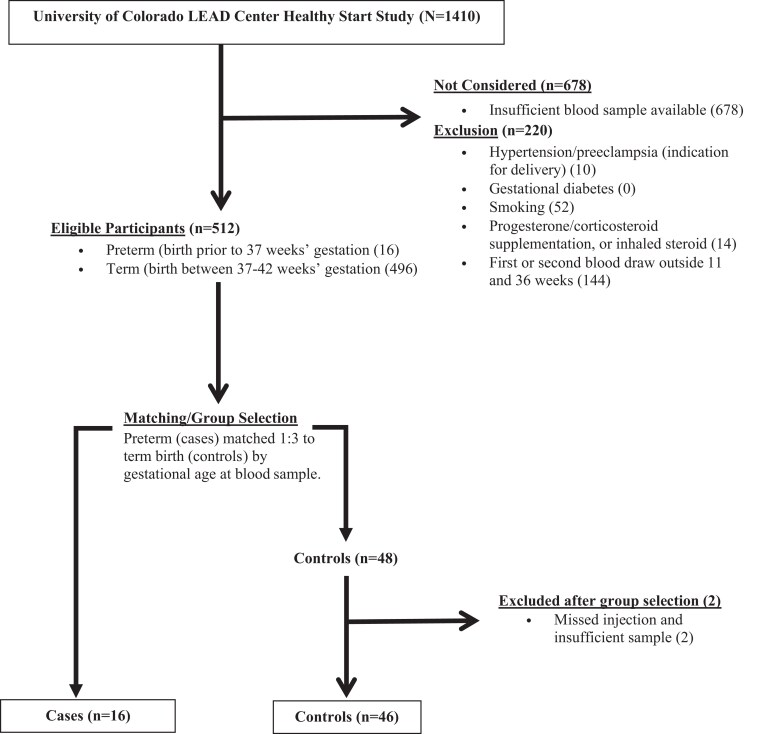
Methods: We performed a nested case-control study using biobanked fasting maternal plasma. We included low-risk singleton pregnancies, and matched 1:3 (16 preterm, 46 term). We quantified high molecular weight (HMW), low molecular weight (LMW), and total adiponectin using an enzyme-linked immunosorbent assay. We validated a high-performance liquid chromatography-tandem mass spectrometry serum assay for use in plasma, to simultaneously measure cortisol, cortisone, and 5 related steroid hormones. We used linear/logistic regression to compare group means and machine learning for predictive modeling.
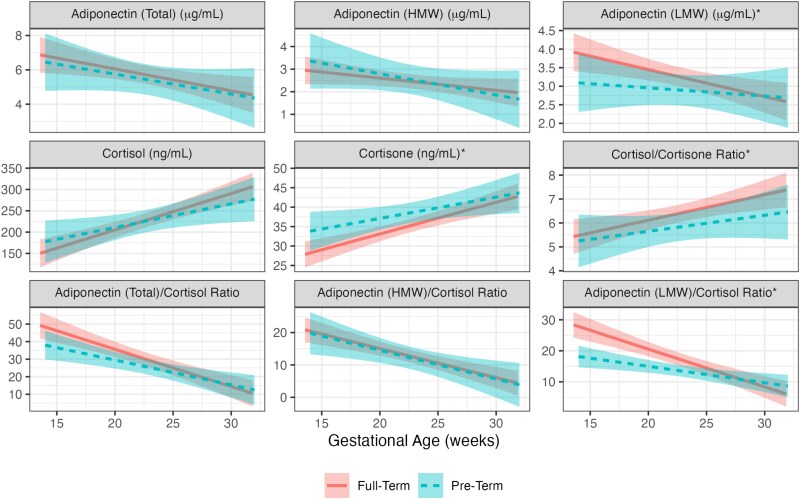
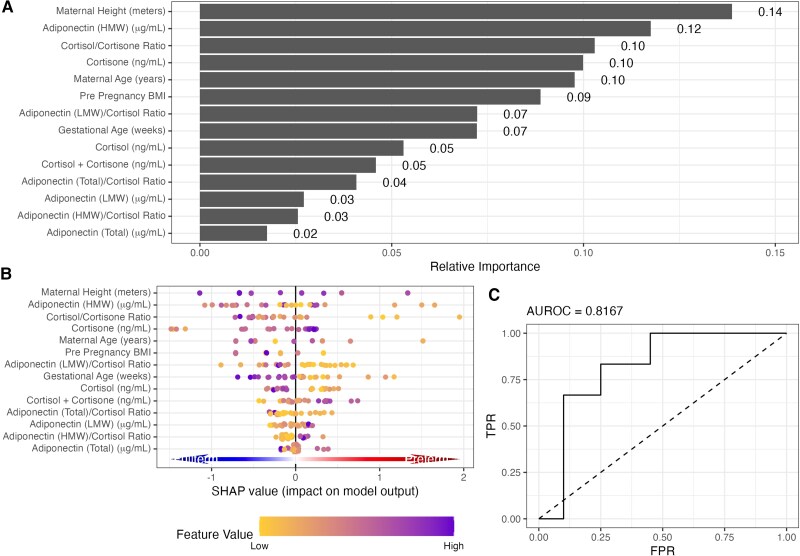
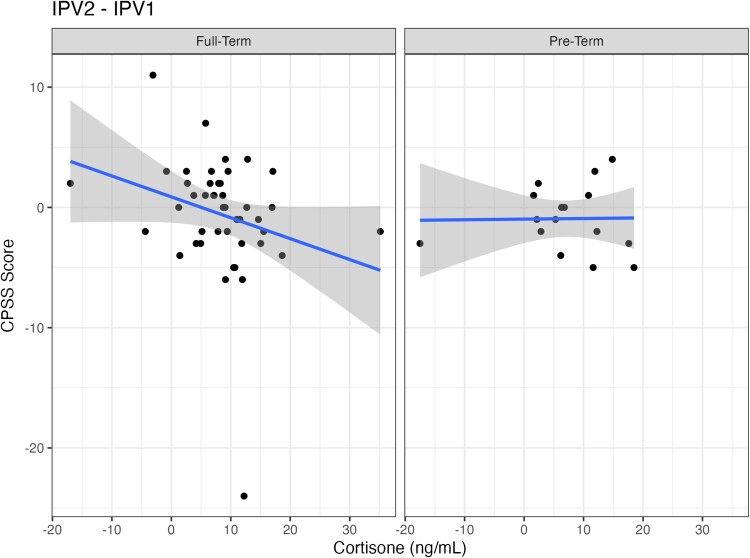
Results: The preterm group had lower mean LMW adiponectin (3.07 μg/mL vs 3.81 μg/mL at 15 weeks (w) 0 days (d), P = .045) and higher mean cortisone (34.4 ng/mL vs 29.0 ng/mL at 15w0d, P = .031). The preterm group had lower cortisol to cortisone and lower LMW adiponectin to cortisol ratios. We found HMW adiponectin, cortisol to cortisone ratio, cortisone, maternal height, age, and prepregnancy body mass index most strongly predicted preterm birth (area under the receiver operator curve = 0.8167). In secondary analyses, we assessed biomarker associations with maternal self-reported psychosocial stress. Lower perceived stress was associated with a steeper change in cortisone in the term group.
Conclusion: Overall, metabolic and stress biomarkers are associated with preterm birth in this healthy cohort. We identify a possible mechanistic link between maternal stress and metabolism for pregnancy maintenance.
Keywords: Cohen's Perceived Stress Scale; Edinburgh Perinatal/Postnatal Depression Scale; adipokine; neuroactive steroid measurement; neuroendocrine; steroid hormone measurement.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com. See the journal About page for additional terms.
Figures
Similar articles
-
A Nested Case-Control Study of Allopregnanolone and Preterm Birth in the Healthy Start Cohort.J Endocr Soc. 2022 Nov 24;7(2):bvac179. doi: 10.1210/jendso/bvac179. eCollection 2022 Dec 15. J Endocr Soc. 2022. PMID: 36632210 Free PMC article.
-
Maternal stress and placental function, a study using questionnaires and biomarkers at birth.PLoS One. 2018 Nov 15;13(11):e0207184. doi: 10.1371/journal.pone.0207184. eCollection 2018. PLoS One. 2018. PMID: 30439989 Free PMC article.
-
Maternal stress/distress, hormonal pathways and spontaneous preterm birth.Paediatr Perinat Epidemiol. 2013 May;27(3):237-46. doi: 10.1111/ppe.12042. Epub 2013 Mar 4. Paediatr Perinat Epidemiol. 2013. PMID: 23574411
-
Are maternal cortisol levels related to preterm birth?J Obstet Gynecol Neonatal Nurs. 2009 Jul-Aug;38(4):377-90. doi: 10.1111/j.1552-6909.2009.01034.x. J Obstet Gynecol Neonatal Nurs. 2009. PMID: 19614873 Review.
-
Omega-3 fatty acid addition during pregnancy.Cochrane Database Syst Rev. 2018 Nov 15;11(11):CD003402. doi: 10.1002/14651858.CD003402.pub3. Cochrane Database Syst Rev. 2018. PMID: 30480773 Free PMC article.
Cited by
-
Stress-induced developmental plasticity and spontaneous preterm birth: A justice-oriented eco-evo-devo review.Eur J Obstet Gynecol Reprod Biol X. 2025 Jun 8;27:100409. doi: 10.1016/j.eurox.2025.100409. eCollection 2025 Sep. Eur J Obstet Gynecol Reprod Biol X. 2025. PMID: 40586095 Free PMC article. Review.
References
-
- Purisch SE, Gyamfi-Bannerman C. Epidemiology of preterm birth. Semin Perinatol. 2017;41(7):387‐391. - PubMed
-
- Hamilton BE, Martin JA, Osterman MJK. Births: provisional data for 2023. Vital Statistics Rapid Release. Report No. 35. April 2024. doi:10.15620/cdc/151797. - DOI
-
- Shapiro-Mendoza CK, Barfield WD, Henderson Z, et al. CDC grand rounds: public health strategies to prevent preterm birth. MMWR Morb Mortal Wkly Rep. 2016;65(32):826‐830. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
