

Predictive Accuracy of the Quick Sepsis-related Organ Failure Assessment Score in Brazil. A Prospective Multicenter Study
- PMID: 31910037
- PMCID: PMC7124712
- DOI: 10.1164/rccm.201905-0917OC
Predictive Accuracy of the Quick Sepsis-related Organ Failure Assessment Score in Brazil. A Prospective Multicenter Study
Abstract
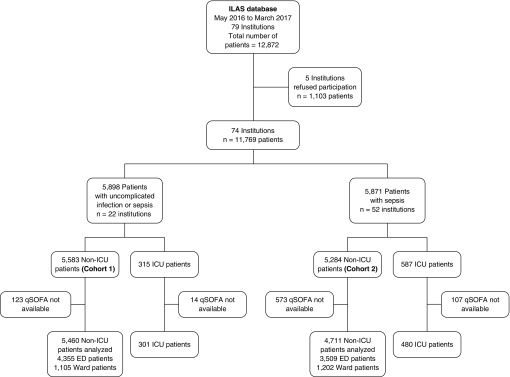
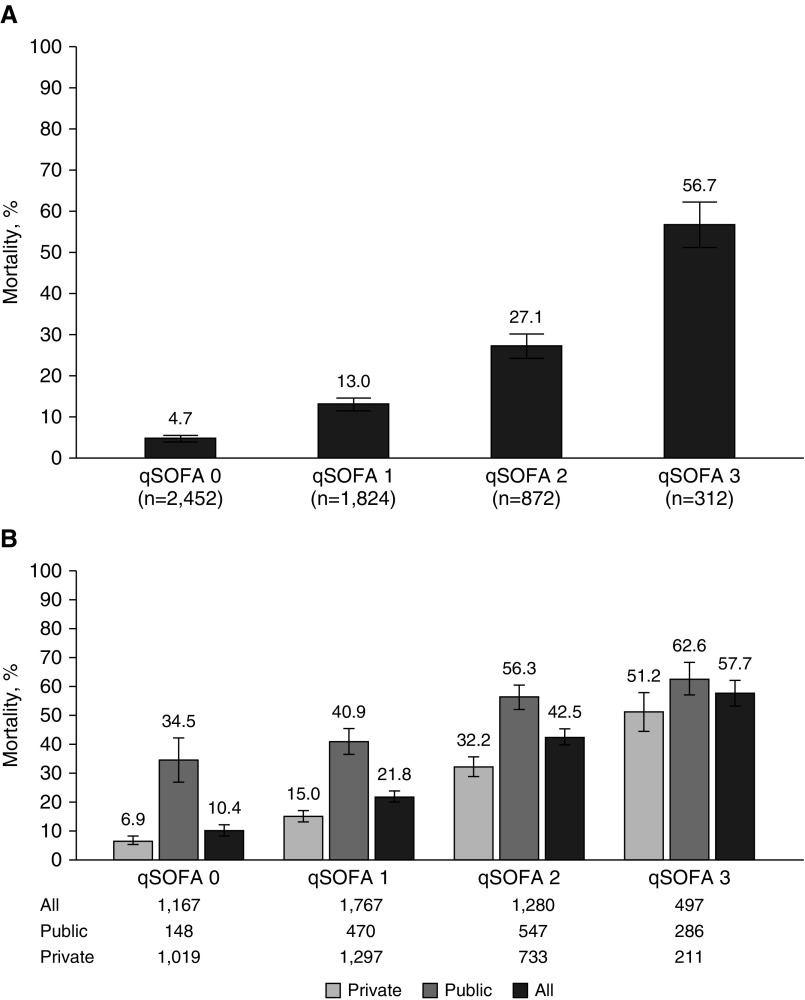
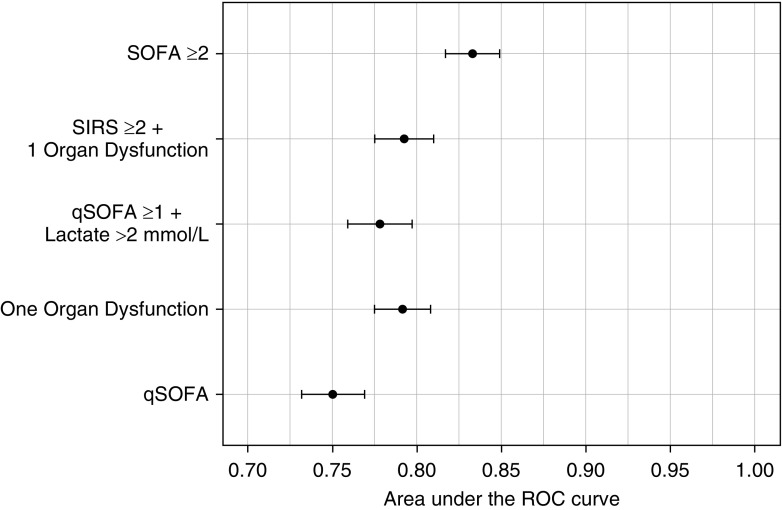
Rationale: Although proposed as a clinical prompt to sepsis based on predictive validity for mortality, the Quick Sepsis-related Organ Failure Assessment (qSOFA) score is often used as a screening tool, which requires high sensitivity.Objectives: To assess the predictive accuracy of qSOFA for mortality in Brazil, focusing on sensitivity.Methods: We prospectively collected data from two cohorts of emergency department and ward patients. Cohort 1 included patients with suspected infection but without organ dysfunction or sepsis (22 hospitals: 3 public and 19 private). Cohort 2 included patients with sepsis (54 hospitals: 24 public and 28 private). The primary outcome was in-hospital mortality. The predictive accuracy of qSOFA was examined considering only the worst values before the suspicion of infection or sepsis.Measurements and Main Results: Cohort 1 contained 5,460 patients (mortality rate, 14.0%; 95% confidence interval [CI], 13.1-15.0), among whom 78.3% had a qSOFA score less than or equal to 1 (mortality rate, 8.3%; 95% CI, 7.5-9.1). The sensitivity of a qSOFA score greater than or equal to 2 for predicting mortality was 53.9% and the 95% CI was 50.3 to 57.5. The sensitivity was higher for a qSOFA greater than or equal to 1 (84.9%; 95% CI, 82.1-87.3), a qSOFA score greater than or equal to 1 or lactate greater than 2 mmol/L (91.3%; 95% CI, 89.0-93.2), and systemic inflammatory response syndrome plus organ dysfunction (68.7%; 95% CI, 65.2-71.9). Cohort 2 contained 4,711 patients, among whom 62.3% had a qSOFA score less than or equal to 1 (mortality rate, 17.3%; 95% CI, 15.9-18.7), whereas in public hospitals the mortality rate was 39.3% (95% CI, 35.5-43.3).Conclusions: A qSOFA score greater than or equal to 2 has low sensitivity for predicting death in patients with suspected infection in a developing country. Using a qSOFA score greater than or equal to 2 as a screening tool for sepsis may miss patients who ultimately die. Using a qSOFA score greater than or equal to 1 or adding lactate to a qSOFA score greater than or equal to 1 may improve sensitivity.Clinical trial registered with www.clinicaltrials.gov (NCT03158493).
Keywords: Quick Sepsis-related Organ Failure Assessment; Sepsis-related Organ Failure Assessment; organ dysfunction; sepsis; systemic inflammatory response syndrome.
Figures
Comment in
-
The Quick Sepsis-related Organ Failure Assessment Score in Brazil: Insights for Future Use in Diverse Settings.Am J Respir Crit Care Med. 2020 Apr 1;201(7):755-756. doi: 10.1164/rccm.202001-0058ED. Am J Respir Crit Care Med. 2020. PMID: 31968174 Free PMC article. No abstract available.
-
In Search of the Ideal Risk Score in Sepsis.Am J Respir Crit Care Med. 2020 Jul 1;202(1):152-153. doi: 10.1164/rccm.202002-0315LE. Am J Respir Crit Care Med. 2020. PMID: 32250644 Free PMC article. No abstract available.
-
Could the Quick Sequential Organ Failure Assessment Predictive Accuracy Be Affected by Site of Infection?Am J Respir Crit Care Med. 2020 Jul 1;202(1):153-154. doi: 10.1164/rccm.202003-0552LE. Am J Respir Crit Care Med. 2020. PMID: 32250647 Free PMC article. No abstract available.
-
Reply to Topeli et al. and to Akinosoglou et al.Am J Respir Crit Care Med. 2020 Jul 1;202(1):154. doi: 10.1164/rccm.202003-0628LE. Am J Respir Crit Care Med. 2020. PMID: 32250649 Free PMC article. No abstract available.
References
-
- Gobatto AL, Besen BA, Azevedo LC. How can we estimate sepsis incidence and mortality? Shock. 2017;47(Suppl 1):6–11. - PubMed
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA. 2014;311:1308–1316. - PubMed
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. International Forum of Acute Care Trialists. Assessment of global incidence and mortality of hospital-treated sepsis: current estimates and limitations. Am J Respir Crit Care Med. 2016;193:259–272. - PubMed
-
- Finfer S, Machado FR. The global epidemiology of sepsis: does it matter that we know so little? Am J Respir Crit Care Med. 2016;193:228–230. - PubMed
-
- Machado FR, Cavalcanti AB, Bozza FA, Ferreira EM, Angotti Carrara FS, Sousa JL, et al. SPREAD Investigators; Latin American Sepsis Institute Network. The epidemiology of sepsis in Brazilian intensive care units (the Sepsis PREvalence Assessment Database, SPREAD): an observational study. Lancet Infect Dis. 2017;17:1180–1189. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
