

Diagnostic uncertainty presented barriers to the timely management of acute thrombotic thrombocytopenic purpura in the United Kingdom between 2014 and 2019
- PMID: 35189012
- PMCID: PMC9314944
- DOI: 10.1111/jth.15681
Diagnostic uncertainty presented barriers to the timely management of acute thrombotic thrombocytopenic purpura in the United Kingdom between 2014 and 2019
Abstract
Background: Acute thrombotic thrombocytopenic purpura (TTP) is a life-threatening emergency and plasma exchange (PEX) is the initial treatment shown to reduce acute mortality.
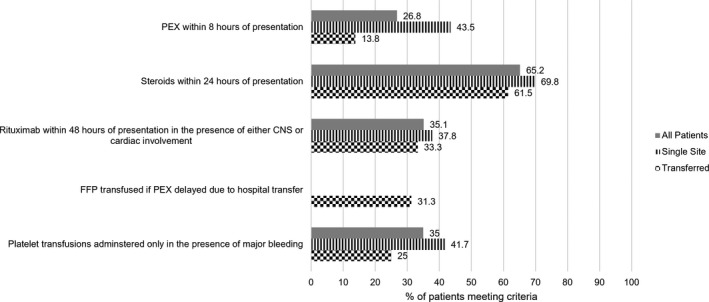
Objectives: To compare current practice in the United Kingdom (UK) against the standards set out in the 2012 British Society of Haematology guideline, and to better understand the issues affecting prompt initiation of PEX.
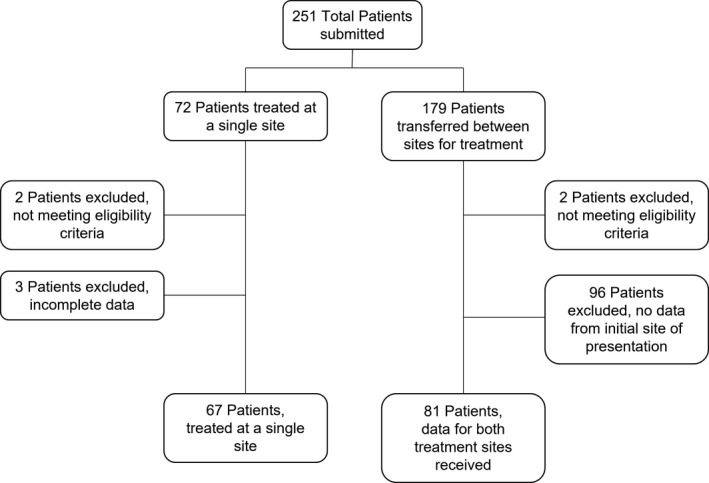
Patients/methods: The trainee research network HaemSTAR conducted a retrospective nationwide review of adults presenting to UK hospitals with a first episode of acute TTP.
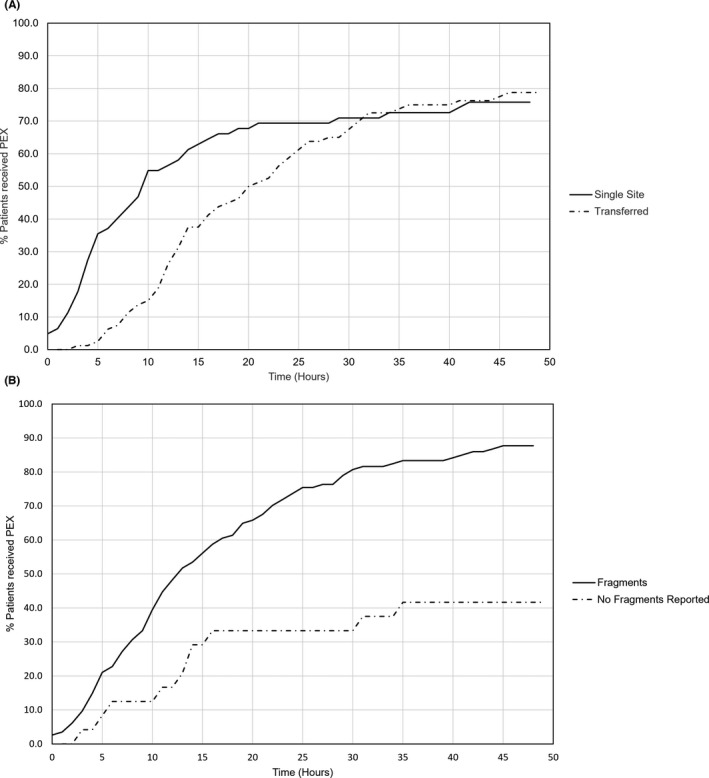
Results: Data on 148 patients treated at 80 UK hospitals between 2014 and 2019 demonstrated that 64.8% of patients received PEX within 24 h. Diagnostic uncertainty was the most commonly cited reason for delayed treatment. Conversely, a shorter time to PEX occurred in patients who had red cell fragments or severe thrombocytopenia identified on their first complete blood count. Availability of on-site PEX was associated with a greater proportion of patients receiving PEX within 8 h compared to patients transferred, but by 24 h there was no difference between the two groups and two-thirds of all patients had received their first PEX. The mortality rate for patients that received PEX was 9.2%, with 27.8% of deaths linked to delayed treatment initiation.
Conclusions: This is the first multi-center evaluation of treatment delays in acute TTP and it will inform targeted pathways to improve prompt access to life-saving intervention.
Keywords: immune thrombotic thrombocytopenic purpura; plasma exchange; quality improvement; service evaluation; thrombocytopenia.
© 2022 The Authors. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Conflict of interest statement
TB has no conflicts of interest to declare. RM has received research funding and honorarium from Sanofi. AD has no conflicts of interest to declare. PLRN has received research grants from Novartis, Principia, and Rigel Pharmaceuticals, as well as honoraria from Bayer, Grifols, and Takeda. RS has no conflicts of interest to declare. AL has no conflicts of interest to declare. ZS has received honoraria from the British Journal of Cardiology. DT has been on advisory boards for Immunovant, Roche, Abbvie, and Novartis; as well as received honoraria for conferences from Amgen and Takeda. MS has received speaker’s fees and advisory boards for Sanofi, Takeda, Octapharma, Novartis, Alexion.
Figures
References
-
- George J. TTP: the evolution of clinical practice. Blood. 2021;137(6):719‐720. - PubMed
-
- Rock GA, Shumak KH, Buskard NA, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med. 1991;325:393‐397. - PubMed
-
- Scully M, Yarranton H, Liesner R, et al. Regional UK TTP registry: correlation with laboratory ADAMTS13 analysis and clinical features. Br J Haematol. 2008;142:819‐826. - PubMed
-
- Dutt T, Scully M. A proposal: the need for thrombotic thrombocytopenic purpura Specialist Centres – providing better outcomes. Br J Haematol. 2015;170:737‐742. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
