

Risk factors for developing ventilator-associated lower respiratory tract infection in patients with severe COVID-19: a multinational, multicentre study, prospective, observational study
- PMID: 37085552
- PMCID: PMC10119842
- DOI: 10.1038/s41598-023-32265-5
Risk factors for developing ventilator-associated lower respiratory tract infection in patients with severe COVID-19: a multinational, multicentre study, prospective, observational study
Abstract
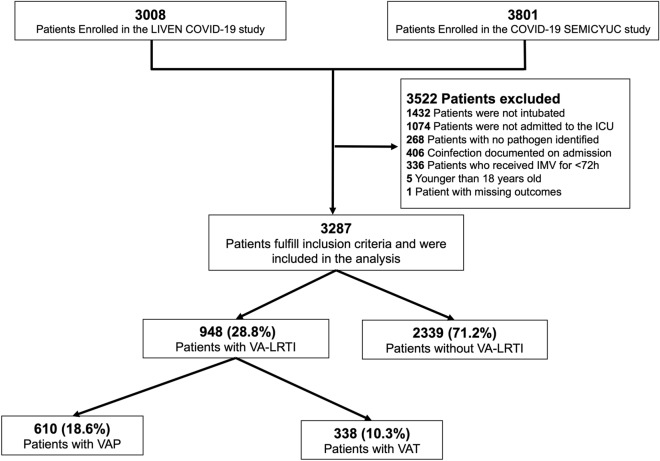
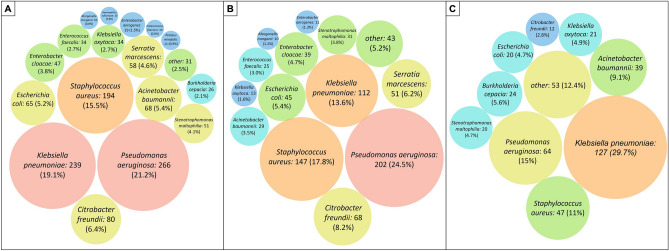
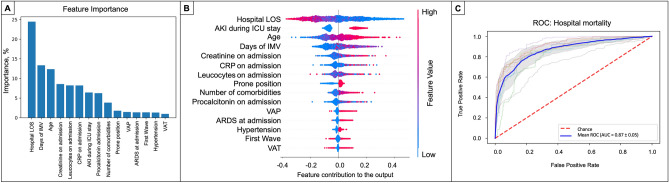
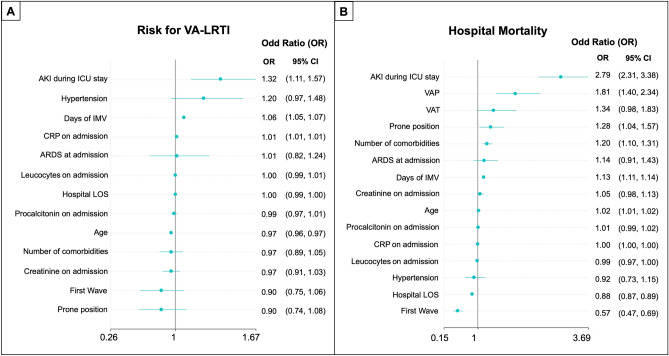
Around one-third of patients diagnosed with COVID-19 develop a severe illness that requires admission to the Intensive Care Unit (ICU). In clinical practice, clinicians have learned that patients admitted to the ICU due to severe COVID-19 frequently develop ventilator-associated lower respiratory tract infections (VA-LRTI). This study aims to describe the clinical characteristics, the factors associated with VA-LRTI, and its impact on clinical outcomes in patients with severe COVID-19. This was a multicentre, observational cohort study conducted in ten countries in Latin America and Europe. We included patients with confirmed rtPCR for SARS-CoV-2 requiring ICU admission and endotracheal intubation. Only patients with a microbiological and clinical diagnosis of VA-LRTI were included. Multivariate Logistic regression analyses and Random Forest were conducted to determine the risk factors for VA-LRTI and its clinical impact in patients with severe COVID-19. In our study cohort of 3287 patients, VA-LRTI was diagnosed in 28.8% [948/3287]. The cumulative incidence of ventilator-associated pneumonia (VAP) was 18.6% [610/3287], followed by ventilator-associated tracheobronchitis (VAT) 10.3% [338/3287]. A total of 1252 bacteria species were isolated. The most frequently isolated pathogens were Pseudomonas aeruginosa (21.2% [266/1252]), followed by Klebsiella pneumoniae (19.1% [239/1252]) and Staphylococcus aureus (15.5% [194/1,252]). The factors independently associated with the development of VA-LRTI were prolonged stay under invasive mechanical ventilation, AKI during ICU stay, and the number of comorbidities. Regarding the clinical impact of VA-LRTI, patients with VAP had an increased risk of hospital mortality (OR [95% CI] of 1.81 [1.40-2.34]), while VAT was not associated with increased hospital mortality (OR [95% CI] of 1.34 [0.98-1.83]). VA-LRTI, often with difficult-to-treat bacteria, is frequent in patients admitted to the ICU due to severe COVID-19 and is associated with worse clinical outcomes, including higher mortality. Identifying risk factors for VA-LRTI might allow the early patient diagnosis to improve clinical outcomes.Trial registration: This is a prospective observational study; therefore, no health care interventions were applied to participants, and trial registration is not applicable.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Chalmers JD, Crichton ML, Goeminne PC, Cao B, Humbert M, Shteinberg M, Antoniou KM, Ulrik CS, Parks H, Wang C, et al. Management of hospitalised adults with coronavirus disease 2019 (COVID-19): A European Respiratory Society living guideline. Eur. Respir. J. 2021;57(4):1. doi: 10.1183/13993003.00048-2021. - DOI - PMC - PubMed
-
- Gundem T, Olasveengen TM, Hovda KE, Gaustad K, Schondorf C, Rostrup M, Froyshov S, Undseth O, Tonby K, Holten AR, et al. Ventilatory support for hypoxaemic intensive care patients with COVID-19. Tidsskr Nor Laegeforen. 2020;140(11):1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
