

GH deficiency status combined with GH receptor polymorphism affects response to GH in children
- PMID: 26340968
- PMCID: PMC4623334
- DOI: 10.1530/EJE-15-0474
GH deficiency status combined with GH receptor polymorphism affects response to GH in children
Abstract
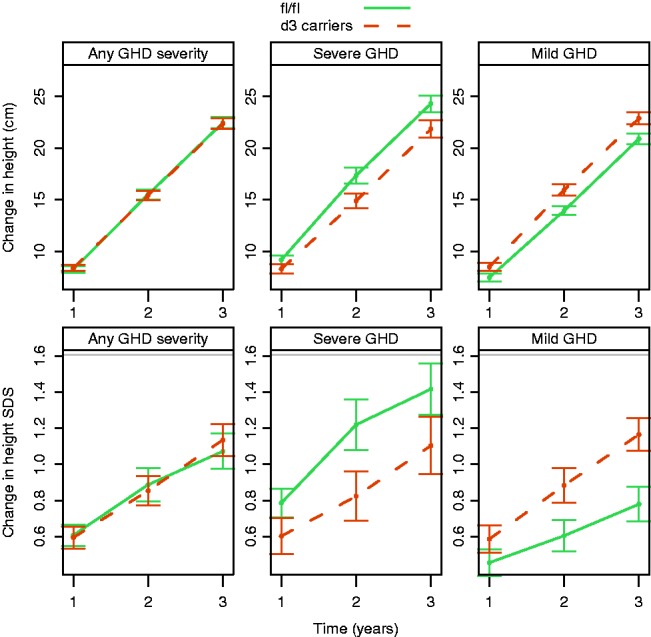
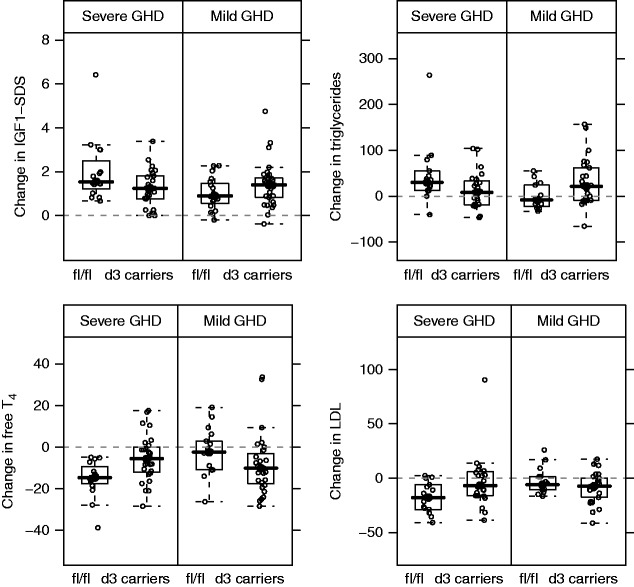
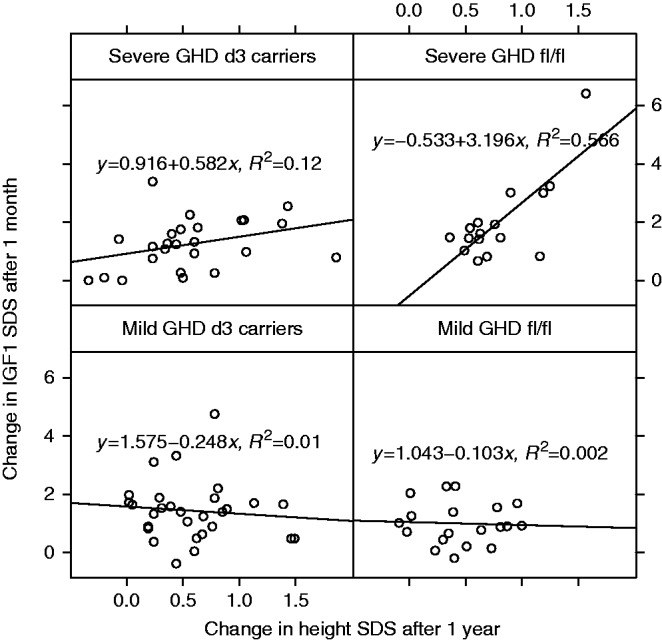
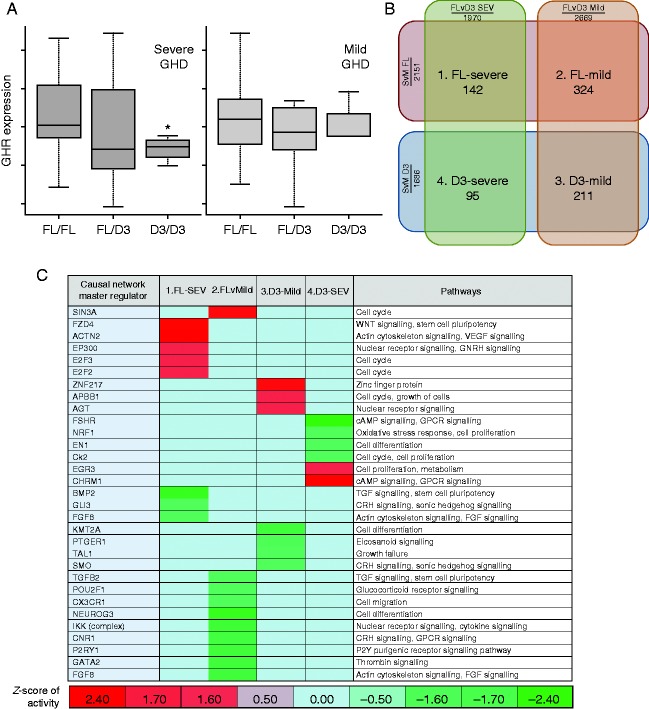
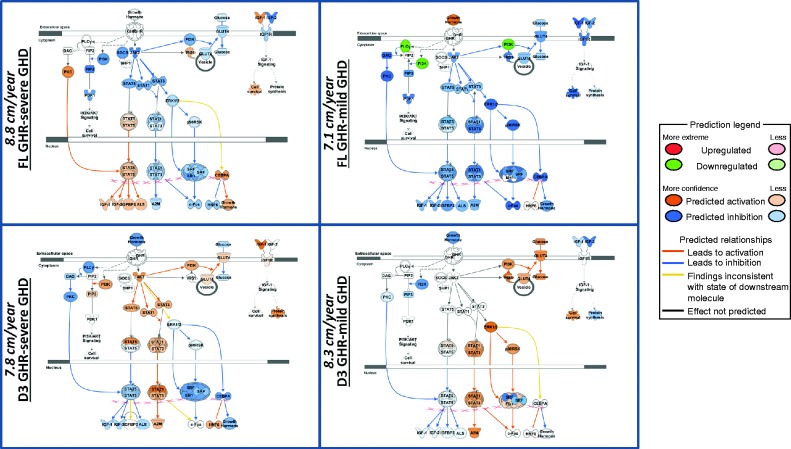
Meta-analysis has shown a modest improvement in first-year growth response to recombinant human GH (r-hGH) for carriers of the exon 3-deleted GH receptor (GHRd3) polymorphism but with significant interstudy variability. The associations between GHRd3 and growth response to r-hGH over 3 years in relation to severity of GH deficiency (GHD) were investigated in patients from 14 countries. Treatment-naïve pre-pubertal children with GHD were enrolled from the PREDICT studies (NCT00256126 and NCT00699855), categorized by peak GH level (peak GH) during provocation test: ≤4 μg/l (severe GHD; n=45) and >4 to <10 μg/l mild GHD; n=49) and genotyped for the GHRd3 polymorphism (full length (fl/fl, fl/d3, d3/d3). Gene expression (GE) profiles were characterized at baseline. Changes in growth (height (cm) and SDS) over 3 years were measured. There was a dichotomous influence of GHRd3 polymorphism on response to r-hGH, dependent on peak GH level. GH peak level (higher vs lower) and GHRd3 (fl/fl vs d3 carriers) combined status was associated with height change over 3 years (P<0.05). GHRd3 carriers with lower peak GH had lower growth than subjects with fl/fl (median difference after 3 years -3.3 cm; -0.3 SDS). Conversely, GHRd3 carriers with higher peak GH had better growth (+2.7 cm; +0.2 SDS). Similar patterns were observed for GH-dependent biomarkers. GE profiles were significantly different between the groups, indicating that the interaction between GH status and GHRd3 carriage can be identified at a transcriptomic level. This study demonstrates that responses to r-hGH depend on the interaction between GHD severity and GHRd3 carriage.
© 2015 The authors.
Figures
References
-
- Binder G, Baur F, Schweizer R, Ranke MB. The d3-growth hormone (GH) receptor polymorphism is associated with increased responsiveness to GH in Turner syndrome and short small-for-gestational-age children. Journal of Clinical Endocrinology and Metabolism. 2006;91:659–664. doi: 10.1210/jc.2005-1581. - DOI - PubMed
-
- Jorge AA, Marchisotti FG, Montenegro LR, Carvalho LR, Mendonca BB, Arnhold IJ. Growth hormone (GH) pharmacogenetics: influence of GH receptor exon 3 retention or deletion on first-year growth response and final height in patients with severe GH deficiency. Journal of Clinical Endocrinology and Metabolism. 2006;91:1076–1080. doi: 10.1210/jc.2005-2005. - DOI - PubMed
-
- Raz B, Janner M, Petkovic V, Lochmatter D, Eble A, Dattani MT, Hindmarsh PC, Fluck CE, Mullis PE. Influence of growth hormone (GH) receptor deletion of exon 3 and full-length isoforms on GH response and final height in patients with severe GH deficiency. Journal of Clinical Endocrinology and Metabolism. 2008;93:974–980. doi: 10.1210/jc.2007-1382. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
