

Intensive Care in India in 2018-2019: The Second Indian Intensive Care Case Mix and Practice Patterns Study
- PMID: 34916740
- PMCID: PMC8645819
- DOI: 10.5005/jp-journals-10071-23965
Intensive Care in India in 2018-2019: The Second Indian Intensive Care Case Mix and Practice Patterns Study
Abstract
Background: We aimed to study organizational aspects, case mix, and practices in Indian intensive care units (ICUs) from 2018 to 2019, following the Indian Intensive Care Case Mix and Practice Patterns Study (INDICAPS) of 2010-2011.
Methods: An observational, 4-day point prevalence study was performed between 2018 and 2019. ICU, patient characteristics, and interventions were recorded for 24 hours, and ICU outcomes till 30 days after the study day. Adherence to selected compliance measures was determined. Data were analyzed for 4,669 adult patients from 132 ICUs.
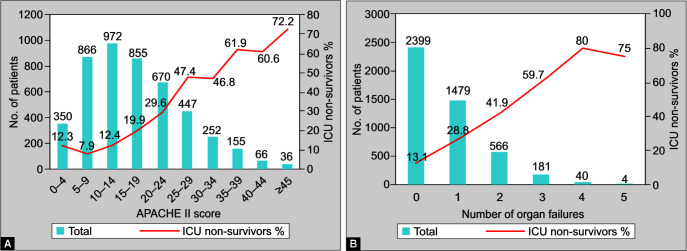
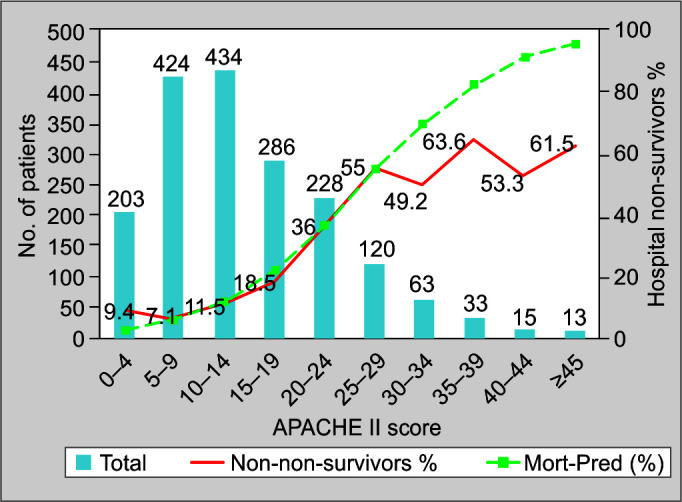
Results: On the study day, mean age, acute physiology and chronic health evaluation (APACHE II), and sequential organ failure assessment (SOFA) scores were 56.9 ± 17.41 years, 16.7 ± 9.8, and 4.4 ± 3.6, respectively. Moreover, 24% and 22.2% of patients received mechanical ventilation (MV) and vasopressors or inotropes (VIs), respectively. On the study days, 1,195 patients (25.6%) were infected and 1,368 patients (29.3%) had sepsis during their ICU stay. ICU mortality was 1,092 out of 4,669 (23.4%), including 737 deaths and 355 terminal discharges (TDs) from ICU. Compliance for process measures related to MV ranged between 62.7 and 85.3%, 11.2 and 47.4% for monitoring delirium, sedation, and analgesia, and 7.7 and 25.3% for inappropriate transfusion of blood products. Only 34.8% of ICUs routinely used capnography. Large hospitals with ≥500 beds, closed ICUs, the APACHE II and SOFA scores, medical admissions, the presence of cancer or cirrhosis of the liver, the presence of infection on the study day, and the need for MV or VIs were independent predictors of mortality.
Conclusions: Hospital size and closed ICUs are independently associated with worse outcomes. The proportion of TDs remains high. There is a scope for improvements in processes of care.Registered at clinicaltrials.gov (NCT03631927).
How to cite this article: Divatia JV, Mehta Y, Govil D, Zirpe K, Amin PR, Ramakrishnan N, et al. Intensive Care in India in 2018-2019: The Second Indian Intensive Care Case Mix and Practice Patterns Study. Indian J Crit Care Med 2021;25(10):1093-1107.
Keywords: Adult; Health care; India; Intensive care units; Mortality; Patients; Process assessment.
Copyright © 2021; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: This study was funded by the Indian Society of Critical Care Medicine Conflict of interest: None
Figures
References
-
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials