

Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): a global, double-blind, randomised, phase 3 trial
- PMID: 30522922
- PMCID: PMC6436818
- DOI: 10.1016/S0140-6736(18)32984-2
Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): a global, double-blind, randomised, phase 3 trial
Erratum in
-
Department of Error.Lancet. 2019 Jan 19;393(10168):228. doi: 10.1016/S0140-6736(18)33123-4. Lancet. 2019. PMID: 30663593 No abstract available.
Abstract
Background: Based on the encouraging activity and manageable safety profile observed in a phase 1 study, the ECHELON-2 trial was initiated to compare the efficacy and safety of brentuximab vedotin, cyclophosphamide, doxorubicin, and prednisone (A+CHP) versus cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) for the treatment of CD30-positive peripheral T-cell lymphomas.
Methods: ECHELON-2 is a double-blind, double-dummy, randomised, placebo-controlled, active-comparator phase 3 study. Eligible adults from 132 sites in 17 countries with previously untreated CD30-positive peripheral T-cell lymphomas (targeting 75% with systemic anaplastic large cell lymphoma) were randomly assigned 1:1 to receive either A+CHP or CHOP for six or eight 21-day cycles. Randomisation was stratified by histological subtype according to local pathology assessment and by international prognostic index score. All patients received cyclophosphamide 750 mg/m2 and doxorubicin 50 mg/m2 on day 1 of each cycle intravenously and prednisone 100 mg once daily on days 1 to 5 of each cycle orally, followed by either brentuximab vedotin 1·8 mg/kg and a placebo form of vincristine intravenously (A+CHP group) or vincristine 1·4 mg/m2 and a placebo form of brentuximab vedotin intravenously (CHOP group) on day 1 of each cycle. The primary endpoint, progression-free survival according to blinded independent central review, was analysed by intent-to-treat. This trial is registered with ClinicalTrials.gov, number NCT01777152.
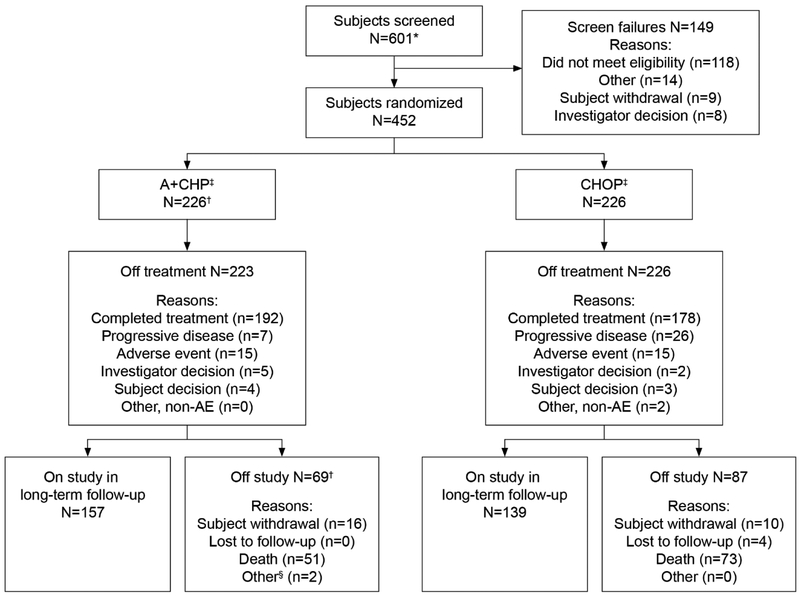
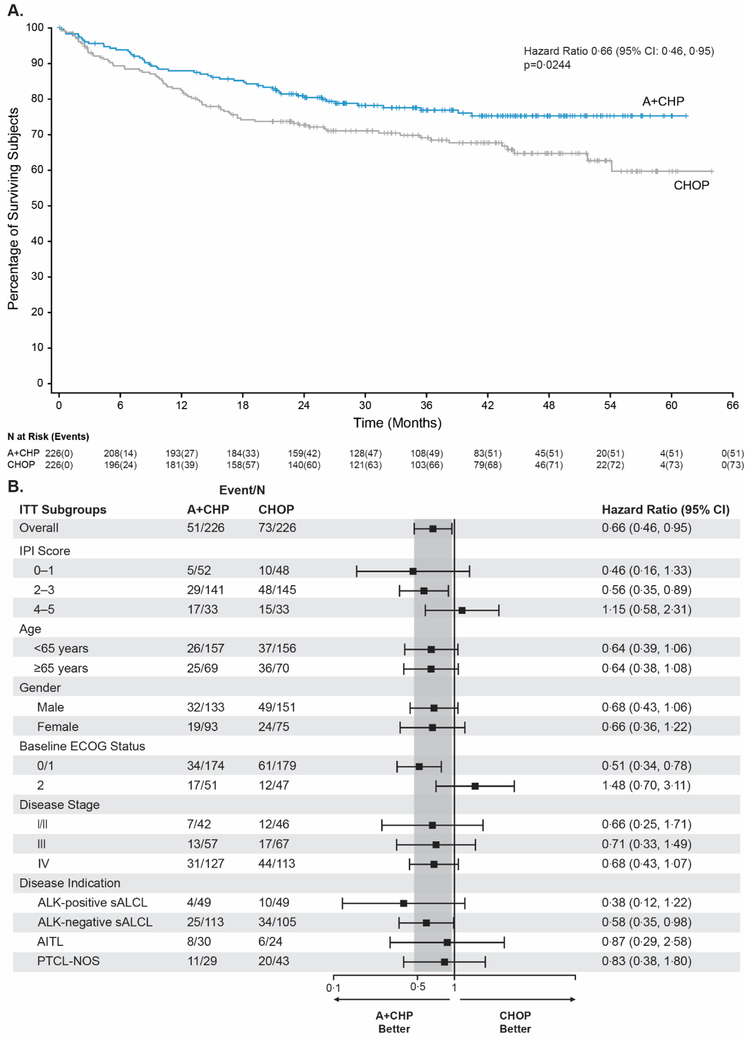
Findings: Between Jan 24, 2013, and Nov 7, 2016, 601 patients assessed for eligibility, of whom 452 patients were enrolled and 226 were randomly assigned to both the A+CHP group and the CHOP group. Median progression-free survival was 48·2 months (95% CI 35·2-not evaluable) in the A+CHP group and 20·8 months (12·7-47·6) in the CHOP group (hazard ratio 0·71 [95% CI 0·54-0·93], p=0·0110). Adverse events, including incidence and severity of febrile neutropenia (41 [18%] patients in the A+CHP group and 33 [15%] in the CHOP group) and peripheral neuropathy (117 [52%] in the A+CHP group and 124 [55%] in the CHOP group), were similar between groups. Fatal adverse events occurred in seven (3%) patients in the A+CHP group and nine (4%) in the CHOP group.
Interpretation: Front-line treatment with A+CHP is superior to CHOP for patients with CD30-positive peripheral T-cell lymphomas as shown by a significant improvement in progression-free survival and overall survival with a manageable safety profile.
Funding: Seattle Genetics Inc, Millennium Pharmaceuticals Inc, a wholly owned subsidiary of Takeda Pharmacuetical Company Limited, and National Institutes of Health National Cancer Institute Cancer Center.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DECLARATION OF INTERESTS
Dr. Horwitz reports receiving grant support from Spectrum, grant support and personal fees from Seattle Genetics, Takeda, Kyowa Hakka Kirin, Verastem Oncology, Aileron, ADC Therapeutics, Celgene, and Forty Seven, and personal fees from Portola, Corvus, Miragen, and Innate; Dr. O’Connor, receiving support from Seattle Genetics to conduct the study; Dr. Pro, receiving grant support and personal fees from Seattle Genetics and personal fees from Takeda; Dr. Illidge, receiving personal fees from Takeda; Dr. Fanale, receiving grant support and personal fees from Seattle Genetics during the conduct of the study, grant support, personal fees, and being employed by and holding shares in Seattle Genetics, grant support and personal fees from Takeda, Celgene, Bristol-Myers Squibb, and Merck, grant support from ADC Therapeutics, MedImmune, Gilead, Molecular Templates, and Genentech, and personal fees from Spectrum and Bayer; Dr. Advani, receiving grant support from Agensys, Celgene, Forty Seven, Infinity, Janssen, Kura Oncology, Merck, Millennium, and Regeneron, grant support and consulting and advisory fees from Bristol Myers Squibb, Genentech/Roche, Pharmacyclics, and Seattle Genetics, consulting and advisory fees from Astra Zeneca, Autolus, Bayer Healthcare Pharmaceuticals, Gilead, Juno, Kite, Kyowa Hakko Kirin, NanoString, Spectrum, Sutro Biopharma, and Takeda, and Data Safety Monitoring Board fees from Cell Medica; Dr. Bartlett, receiving research funding from Celgene, Seattle Genetics, Genentech, Kite, Merck, Bristol-Meyers Squibb, Immune Designs, Forty Seven, Affimed, Janssen, Pharmacyclics, Millennium, and Gilead, and advisory board fees from Acerta and Pfizer; Dr. Christensen has nothing to disclose; Dr. Morschhauser, receiving honoraria from Takeda, advisory board fees from Bristol- Myers Squibb, lecture fees from Janssen, advisory board and lecture fees from Celgene and Roche, consultant fees from Epizyme, and consultant, advisory board, and lecture fees from Gilead; Dr. Domingo-Domenech, receiving non-financial support from Seattle Genetics and personal fees from Bristol-Myers Squibb and Takeda; Dr. Rossi, receiving personal fees from Roche, Celgene, Janssen, Amgen, Gilead, Sanofi, Pfizer, AbbVie, Jazz Pharmaceuticals, Novartis, Bristol-Myers Squibb, and Sandoz; Dr. Kim has nothing to disclose; Dr. Feldman, receiving consultant fees from Bristol-Myers Squibb, speaker’s bureau fees and honoraria from Celgene, Pharmacyclis, Janssen, Kite, and AbbVie, and sponsor support, consultant and speaker’s bureau fees, and honoraria from Seattle Genetics; Dr. Lennard has nothing to disclose; Dr. Belada, receiving research support from Seattle Genetics and consultant and advisory board fees from Takeda; Dr. Illés has nothing to disclose; Dr. Tobinai, receiving grant support from GlaxoSmithKline, Servier, and AbbVie, honoraria from Zenyaku Kogyo, and grant support and honoraria from Takeda, Eisai, Celgene, Mundipharma, Janssen, HUYA Bioscience International, Kyowa Hakko Kirin, Chugai Pharma, and Ono Pharma; Dr. Tsukasaki, receiving grant support from Seattle Genetics and Eisai, consultant fees from Ono Pharma and Daiichi-Sankyo, honoraria from Kyowa Hakko Kirin, grant support and honoraria from Celgene and Chugai Pharma, and grant support, consultant fees, and honoraria from HUYA Bioscience International; Dr. Yeh, has nothing to disclose; Dr. Shustov, receiving research funding from Seattle Genetics; Dr. Hüttmann, receiving grant support, honoraria and drug supply for study conduct from Takeda; Dr. Savage, receiving honoraria and advisory board fees from Seattle Genetics, and honoraria from Takeda during the conduct of the study, honoraria and advisory board frees from Bristol-Myers Squibb, Merck, Verastem, Abbvie, and consulting fees from Servier; Dr. Yuen, has nothing to disclose; Dr. Iyer, receiving grant support from Seattle Genetics, Takeda, Roche, Rhizen, Spectrum, Celgene, Gilead, Novarits, Amgen, and Trillium; Dr. Zinzani, receiving advisory board fees and honoraria from Gilead, Sandoz, Johnson & Johnson, Bristol-Myers Squibb, Servier, Takeda, Celtrion, Roche, and Celgene; Dr. Hua has nothing to disclose; Ms. Little, holding shares in and employment with Takeda; Dr. Rao, being employed by and holding shares in Seattle Genetics; Dr. Woolery, being employed by and holding shares in Seattle Genetics; Dr. Manley, being employed by and holding shares in Seattle Genetics and has a patents 62/580,261, 62/739,631, and 62/739,635 licensed to Takeda (all ex-US, except Canada); and Dr. Trümper, receiving grant support from Seattle Genetics and the German Ministry of Education and Research (Bundesministerium für Bildung und Forschung) and grant and non-financial support from Genzyme. No other potential conflict of interest relevant to this article was reported.
Figures

Comment in
-
Moving to a higher echelon in CD30-positive T-cell lymphoma.Lancet. 2019 Jan 19;393(10168):201-202. doi: 10.1016/S0140-6736(18)33127-1. Lancet. 2019. PMID: 30663580 No abstract available.
-
The upper ECHELON against T-cell lymphoma.Ann Oncol. 2022 Mar;33(3):239-241. doi: 10.1016/j.annonc.2021.12.011. Epub 2022 Jan 10. Ann Oncol. 2022. PMID: 35017032 No abstract available.
References
-
- Horwitz SM, Zelenetz AD, Gordon LI, et al. NCCN Guidelines® insights: Non-Hodgkin's lymphomas, version 3.2016 featured updates to the NCCN guidelines. JNCCN Journal of the National Comprehensive Cancer Network 2016; 14(9): 1067–79. - PubMed
-
- d'Amore F, Gaulard P, Trumper L, et al. Peripheral T-cell lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015; 26 Suppl 5: v108–15. - PubMed
-
- Savage KJ, Chhanabhai M, Gascoyne RD, Connors JM. Characterization of peripheral T-cell lymphomas in a single North American institution by the WHO classification. Ann Oncol 2004; 15(10): 1467–75. - PubMed
-
- Simon A, Peoch M, Casassus P, et al. Upfront VIP-reinforced-ABVD (VIP-rABVD) is not superior to CHOP/21 in newly diagnosed peripheral T cell lymphoma. Results of the randomized phase III trial GOELAMS-LTP95. Br J Haematol 2010; 151(2): 159–66. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
