

Efficacy of Tocilizumab in Patients Hospitalized with Covid-19
- PMID: 33085857
- PMCID: PMC7646626
- DOI: 10.1056/NEJMoa2028836
Efficacy of Tocilizumab in Patients Hospitalized with Covid-19
Abstract
Background: The efficacy of interleukin-6 receptor blockade in hospitalized patients with coronavirus disease 2019 (Covid-19) who are not receiving mechanical ventilation is unclear.
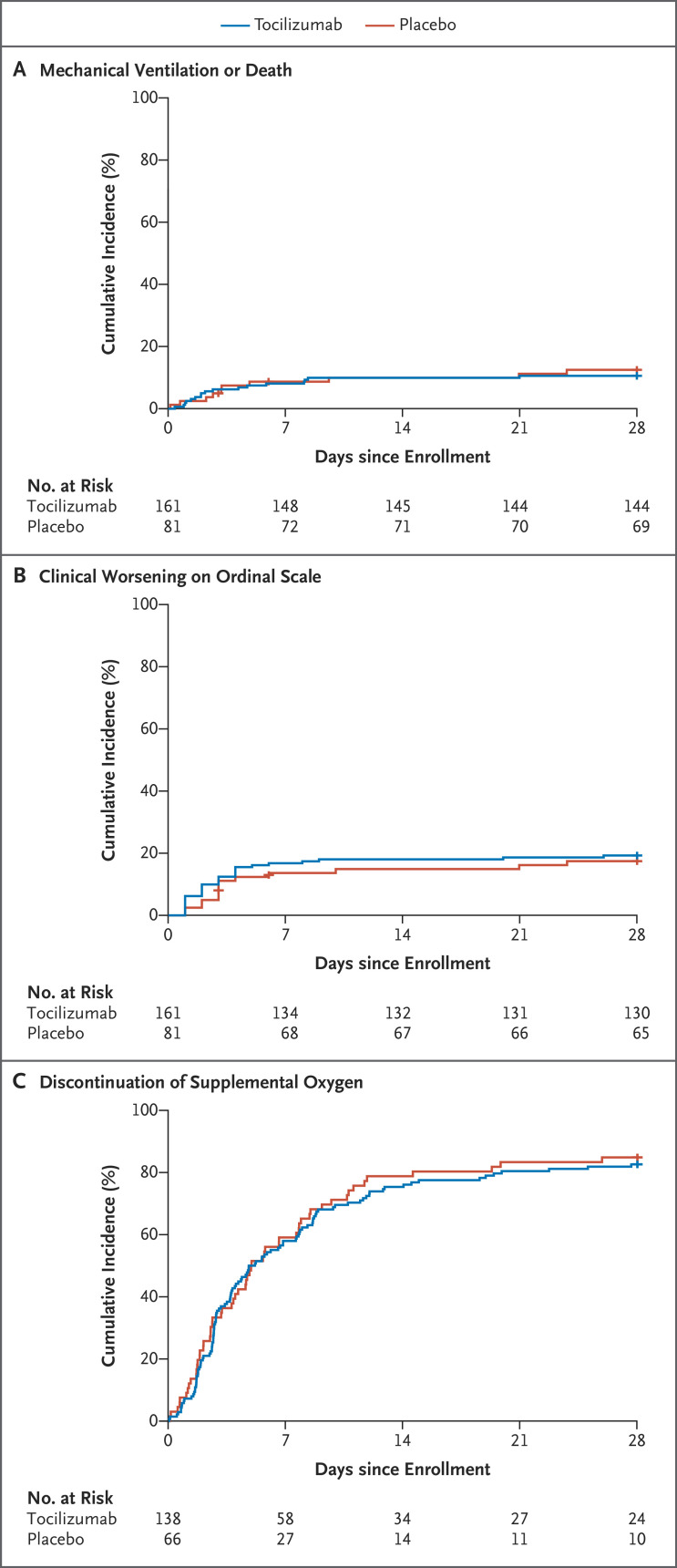
Methods: We performed a randomized, double-blind, placebo-controlled trial involving patients with confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, hyperinflammatory states, and at least two of the following signs: fever (body temperature >38°C), pulmonary infiltrates, or the need for supplemental oxygen in order to maintain an oxygen saturation greater than 92%. Patients were randomly assigned in a 2:1 ratio to receive standard care plus a single dose of either tocilizumab (8 mg per kilogram of body weight) or placebo. The primary outcome was intubation or death, assessed in a time-to-event analysis. The secondary efficacy outcomes were clinical worsening and discontinuation of supplemental oxygen among patients who had been receiving it at baseline, both assessed in time-to-event analyses.
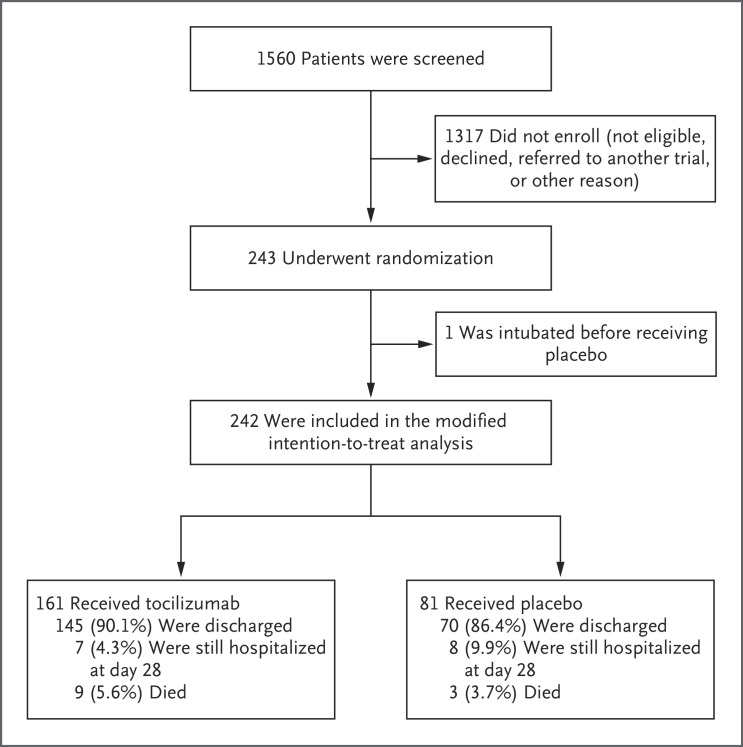
Results: We enrolled 243 patients; 141 (58%) were men, and 102 (42%) were women. The median age was 59.8 years (range, 21.7 to 85.4), and 45% of the patients were Hispanic or Latino. The hazard ratio for intubation or death in the tocilizumab group as compared with the placebo group was 0.83 (95% confidence interval [CI], 0.38 to 1.81; P = 0.64), and the hazard ratio for disease worsening was 1.11 (95% CI, 0.59 to 2.10; P = 0.73). At 14 days, 18.0% of the patients in the tocilizumab group and 14.9% of the patients in the placebo group had had worsening of disease. The median time to discontinuation of supplemental oxygen was 5.0 days (95% CI, 3.8 to 7.6) in the tocilizumab group and 4.9 days (95% CI, 3.8 to 7.8) in the placebo group (P = 0.69). At 14 days, 24.6% of the patients in the tocilizumab group and 21.2% of the patients in the placebo group were still receiving supplemental oxygen. Patients who received tocilizumab had fewer serious infections than patients who received placebo.
Conclusions: Tocilizumab was not effective for preventing intubation or death in moderately ill hospitalized patients with Covid-19. Some benefit or harm cannot be ruled out, however, because the confidence intervals for efficacy comparisons were wide. (Funded by Genentech; ClinicalTrials.gov number, NCT04356937.).
Copyright © 2020 Massachusetts Medical Society.
Conflict of interest statement
Dr. Stone reports receiving grant support and consulting fees from Principia Biopharma and Roche, grant support from Viela, advisory board fees and consulting fees from Sanofi, and consulting fees from Chemocentryx, Celgene, AbbVie, Chugai, Gruenthal, GlaxoSmithKline, InflaRx, INSmed, Regeneron, and Roivant; Dr. Frigault, receiving consulting fees and advisory board fees from Novartis and Celgene/BMS and consulting fees from Kite/Gilead and Arcellx; Dr. Healy, receiving grant support from Analysis Group, Celgene (Bristol-Myers Squibb), Verily Life Sciences, Novartis, Merck Serono, and Genzyme; Dr. Dougan, receiving grant support from Novartis and Eli Lilly, grant support and consulting fees from Genentech, consulting fees from ORIC Pharmaceuticals, Partner Therapeutics, and Tillotts Pharma, and advisory board fees from Neoleukin Therapeutics; Dr. Kim, receiving advisory board fees from Biomarin; Dr. Neilan, receiving consulting fees from Parexel and Intrinsic Imaging, advisory board fees from AbbVie, Bristol-Myers Squibb, and H3 Biomedicine, and grant support from AstraZeneca; Dr. Unizony, receiving consulting fees from Janssen and Kiniksa and grant support from Genentech; Dr. Bolster, receiving grant support from Amgen, AbbVie, Pfizer, Cumberland, and Corbus Pharmaceuticals, advisory board fees from Gilead Sciences, consulting fees from Custom Learning Designs, honoraria from Merck Manual, and investments in Johnson & Johnson; Dr. Mansour, receiving consulting fees from Vericel, SmartPharm Therapeutics, Pulsethera, GenMark Diagnostics, Globe Life Sciences, and Day Zero Diagnostics, grant support from Thermo Fisher Scientific and Genentech, advisory board fees from Celularity, holding pending patent 14/110,443 on fungal particles, and pending patent 15/999,463 on cellular therapy for infections. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Tocilizumab for Covid-19 - The Ongoing Search for Effective Therapies.N Engl J Med. 2020 Dec 10;383(24):2387-2388. doi: 10.1056/NEJMe2032071. N Engl J Med. 2020. PMID: 33296566 Free PMC article. No abstract available.
-
Tocilizumab in Covid-19.N Engl J Med. 2021 Jan 7;384(1):86-87. doi: 10.1056/NEJMc2032911. Epub 2020 Dec 22. N Engl J Med. 2021. PMID: 33356049 No abstract available.
-
Tocilizumab in Patients Hospitalized with Covid-19 Pneumonia.N Engl J Med. 2021 Apr 15;384(15):1473. doi: 10.1056/NEJMc2100217. Epub 2021 Mar 3. N Engl J Med. 2021. PMID: 33657286 No abstract available.
References
-
- Centers for Disease Control. United States COVID-19 cases and deaths by state (https://covid.cdc.gov/covid-data-tracker/).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous