

Neurologic manifestations associated with COVID-19: a multicentre registry
- PMID: 33189873
- PMCID: PMC7661948
- DOI: 10.1016/j.cmi.2020.11.005
Neurologic manifestations associated with COVID-19: a multicentre registry
Abstract
Objectives: To provide an overview of the spectrum, characteristics and outcomes of neurologic manifestations associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Methods: We conducted a single-centre retrospective study during the French coronavirus disease 2019 (COVID-19) epidemic in March-April 2020. All COVID-19 patients with de novo neurologic manifestations were eligible.
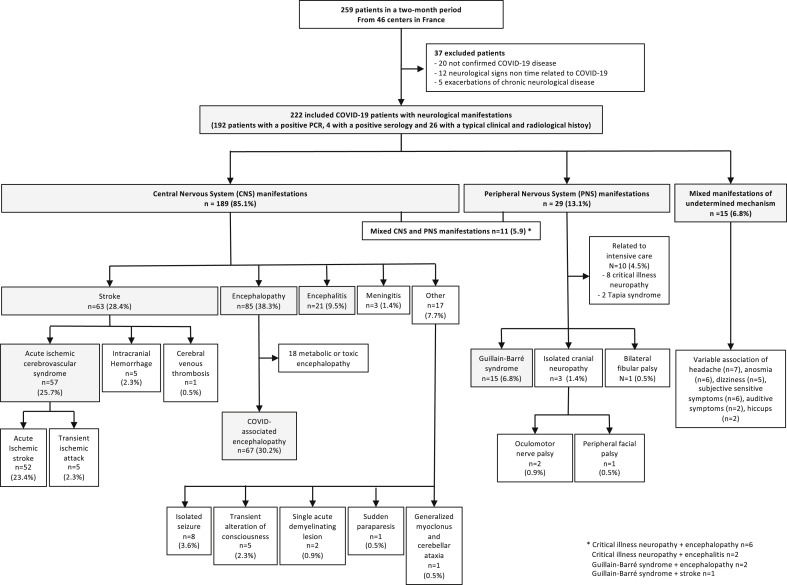
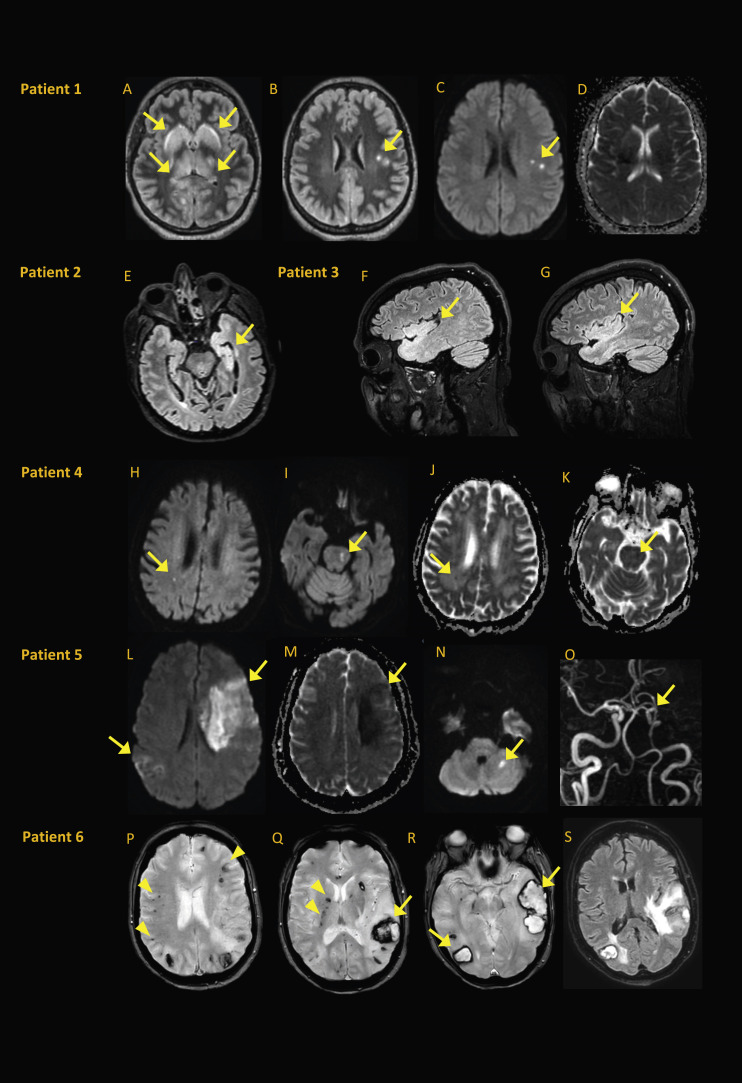
Results: We included 222 COVID-19 patients with neurologic manifestations from 46 centres in France. Median (interquartile range, IQR) age was 65 (53-72) years and 136 patients (61.3%) were male. COVID-19 was severe or critical in 102 patients (45.2%). The most common neurologic diseases were COVID-19-associated encephalopathy (67/222, 30.2%), acute ischaemic cerebrovascular syndrome (57/222, 25.7%), encephalitis (21/222, 9.5%) and Guillain-Barré syndrome (15/222, 6.8%). Neurologic manifestations appeared after the first COVID-19 symptoms with a median (IQR) delay of 6 (3-8) days in COVID-19-associated encephalopathy, 7 (5-10) days in encephalitis, 12 (7-18) days in acute ischaemic cerebrovascular syndrome and 18 (15-28) days in Guillain-Barré syndrome. Brain imaging was performed in 192 patients (86.5%), including 157 magnetic resonance imaging (70.7%). Among patients with acute ischaemic cerebrovascular syndrome, 13 (22.8%) of 57 had multiterritory ischaemic strokes, with large vessel thrombosis in 16 (28.1%) of 57. Brain magnetic resonance imaging of encephalitis patients showed heterogeneous acute nonvascular lesions in 14 (66.7%) of 21. Cerebrospinal fluid of 97 patients (43.7%) was analysed, with pleocytosis found in 18 patients (18.6%) and a positive SARS-CoV-2 PCR result in two patients with encephalitis. The median (IQR) follow-up was 24 (17-34) days with a high short-term mortality rate (28/222, 12.6%).
Conclusions: Clinical spectrum and outcomes of neurologic manifestations associated with SARS-CoV-2 infection were broad and heterogeneous, suggesting different underlying pathogenic processes.
Keywords: COVID-19; Nervous system; Neurologic manifestations; Registry; SARS-CoV-2.
Copyright © 2020 European Society of Clinical Microbiology and Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
