

Efficacy and safety of the SGLT2 inhibitor empagliflozin versus placebo and the DPP-4 inhibitor linagliptin versus placebo in young people with type 2 diabetes (DINAMO): a multicentre, randomised, double-blind, parallel group, phase 3 trial
- PMID: 36738751
- PMCID: PMC10851109
- DOI: 10.1016/S2213-8587(22)00387-4
Efficacy and safety of the SGLT2 inhibitor empagliflozin versus placebo and the DPP-4 inhibitor linagliptin versus placebo in young people with type 2 diabetes (DINAMO): a multicentre, randomised, double-blind, parallel group, phase 3 trial
Abstract
Background: The incidence of type 2 diabetes in young people is increasing, but treatments remain limited. We aimed to assess the efficacy and safety of an empagliflozin dosing regimen versus placebo and linagliptin versus placebo on glycaemic control in young people with type 2 diabetes.
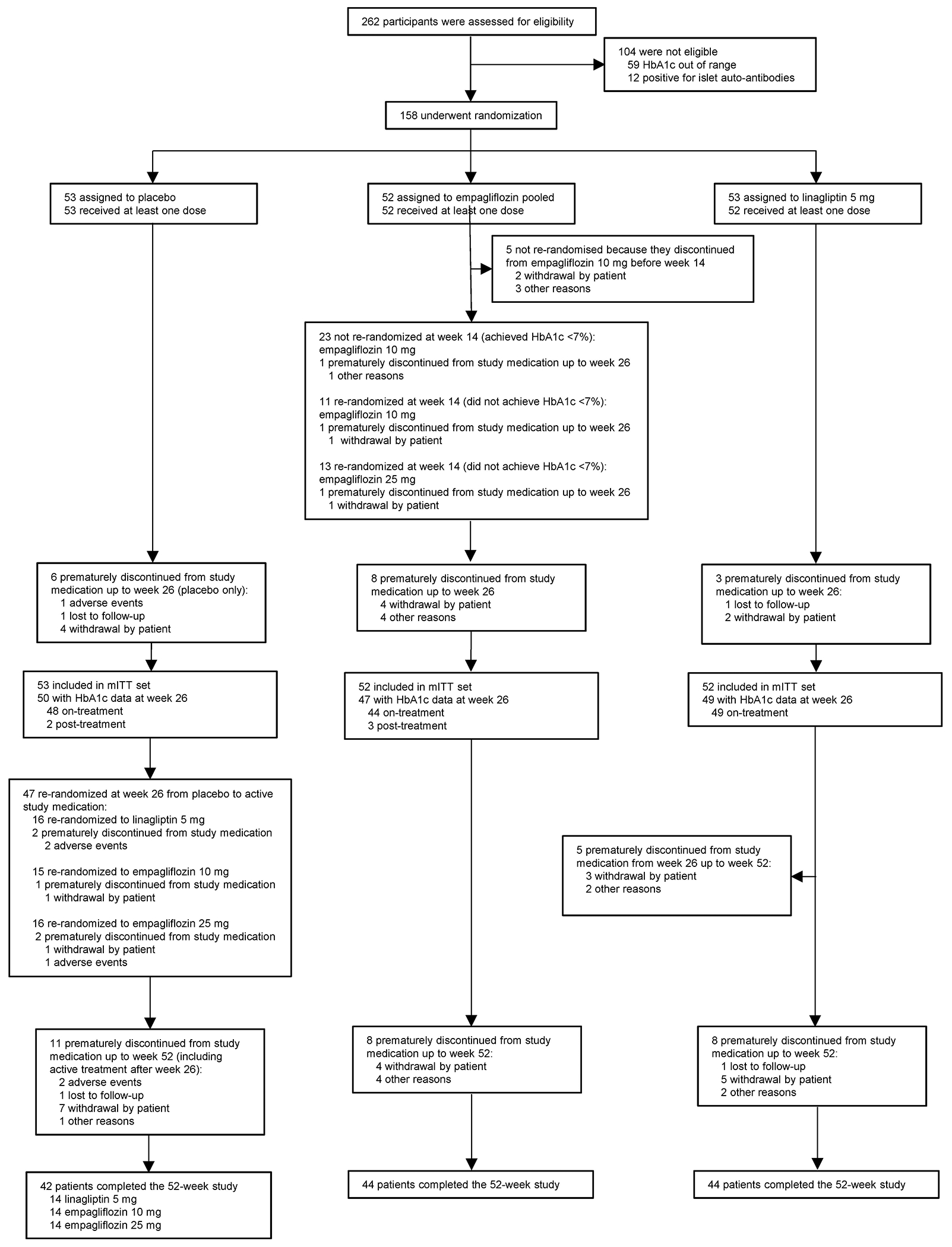
Methods: In this double-blind, placebo-controlled trial done in 108 centres in 15 countries, participants with type 2 diabetes (aged 10-17 years; HbA1c 6·5-10·5% [48-91 mmol/mol]) who had been previously treated with metformin or insulin were randomly assigned (1:1:1) to oral empagliflozin 10 mg, oral linagliptin 5 mg, or placebo. Participants in the empagliflozin group who did not have HbA1c below 7·0% (<53 mmol/mol) by week 12 underwent a second double-blinded randomisation (1:1) at week 14, either remaining on 10 mg or increasing to 25 mg. Participants in the placebo group were randomly reassigned (1:1:1) in a double-blinded manner at week 26 to linagliptin 5 mg or one of the empagliflozin doses (10 mg or 25 mg). Investigators were masked throughout the trial and received assignments of blinded medication kits through interactive response technology for all participants at the initial randomisation and for the re-randomisations at weeks 14 and 26. The primary outcome was change from baseline in HbA1c at 26 weeks. For empagliflozin, results were based on a pooled analysis for all participants on empagliflozin. Safety was assessed until week 52. This trial is registered with ClinicalTrials.gov, NCT03429543.
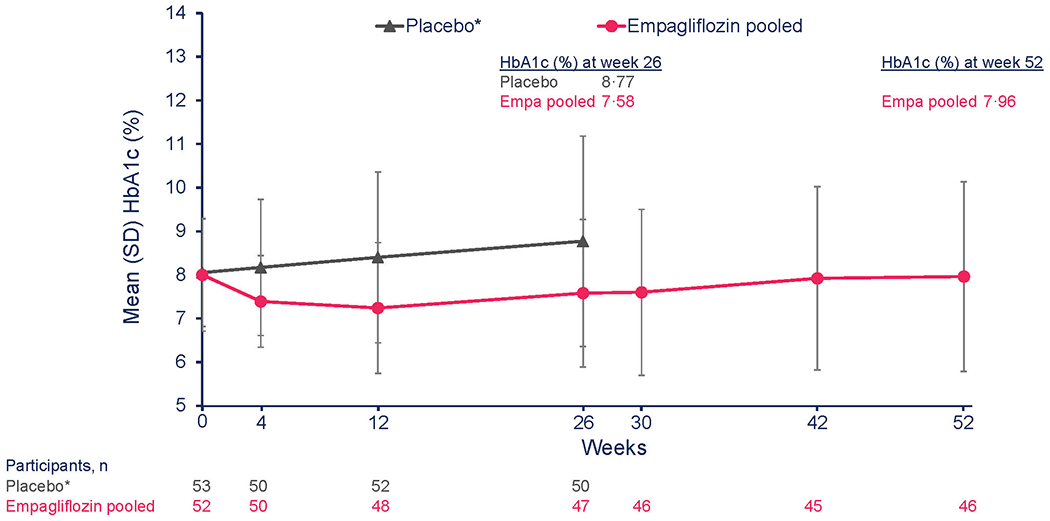
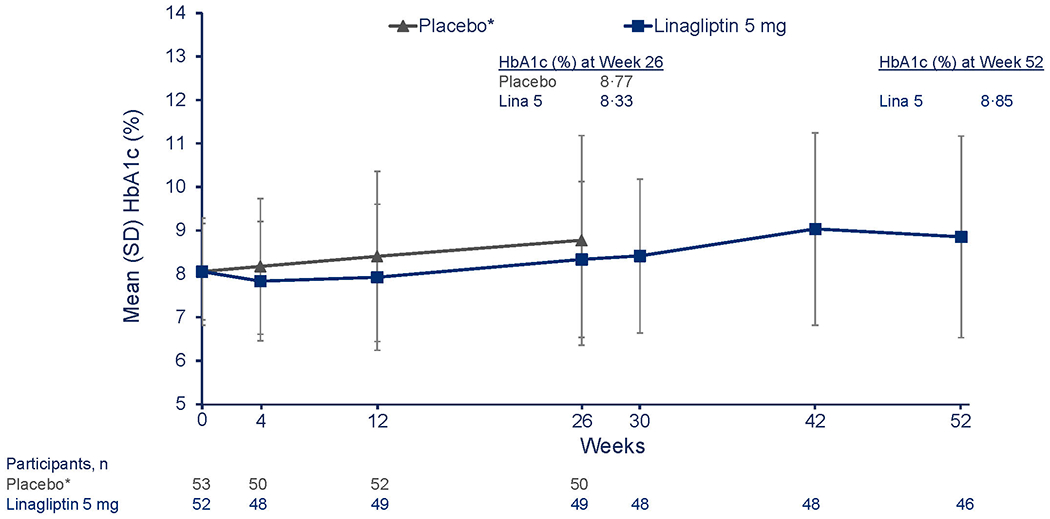
Findings: Between April 26, 2018, and May 26, 2022, of 262 screened participants, 158 (60%) were randomly assigned to treatment (53 [34%] to placebo, 52 [33%] to empagliflozin 10 mg, and 53 [34%] to linagliptin). For the primary outcome, the adjusted mean HbA1c change from baseline at week 26 was -0·84% [-9·2 mmol/mol] in the empagliflozin pooled group versus placebo (95% CI -1·50 to -0·19 [-16·4 to -2·1]; p=0·012); the corresponding change from baseline for linagliptin versus placebo was -0·34% [-3·8 mmol/mol; 95% CI -0·99 to 0·30 [-10·8 to 3·3]; p=0·29). Adverse events occurred in 34 (64%) participants in the placebo group, 40 (77%) in the empagliflozin pooled group, and 37 (71%) in the linagliptin group, up to week 26. Of these, severe adverse events were reported in two (4%) participants in the placebo group, one (2%) in the empagliflozin pooled group, and one (2%) in the linagliptin group. Hypoglycaemia was the most frequently reported adverse event with higher rates for those on active drug treatment compared with placebo. No severe hypoglycaemia cases were reported.
Interpretation: Empagliflozin provided clinically relevant placebo-corrected reductions in HbA1c, whereas linagliptin did not, and might offer a new treatment option for young people with type 2 diabetes.
Funding: The Boehringer Ingelheim and Eli Lilly and Company Alliance.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests LML has received consulting fees from Provention, Dompe, Medtronic, Roche, Janssen, Eli Lilly, Dexcom, Novo Nordisk, and Vertex. TD has received speaker, advisory panel, or research support from AstraZeneca, Bayer, Boehringer Ingelheim, Dexcom, Eli Lilly, Insulet, Lifescan, Medtronic, Novo Nordisk, Roche, and Sanofi; and is a shareholder of DreaMed Diabetes. WVT has received consulting fees from AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Medtronic Diabetes. SW has served on a data safety monitoring board for the National Institute of Diabetes and Digestive and Kidney Diseases/US National Institutes of Health; and served on an advisory panel or board for Roche Diagnostics and Medtronic MiniMed. PZ has consulted for Boehringer Ingelheim, Merck, Eli Lilly, Janssen, I-ACT, and Novo Nordisk. DN and JM are employees of Boehringer Ingelheim. GJK declares no competing interests.
Figures
Comment in
-
Challenges in the treatment of young people with type 2 diabetes.Lancet Diabetes Endocrinol. 2023 Mar;11(3):141-143. doi: 10.1016/S2213-8587(23)00030-X. Epub 2023 Feb 1. Lancet Diabetes Endocrinol. 2023. PMID: 36738752 No abstract available.
References
-
- Darnton-Hill I, Nishida C, James WP. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr 2004; 7(1A): 101–21. - PubMed
-
- Nolan CJ, Damm P, Prentki M. Type 2 diabetes across generations: from pathophysiology to prevention and management. Lancet 2011; 378(9786): 169–81. - PubMed
-
- International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Brussels; 2021.
-
- Al-Saeed AH, Constantino MI, Molyneaux L, et al. An Inverse Relationship Between Age of Type 2 Diabetes Onset and Complication Risk and Mortality: The Impact of Youth-Onset Type 2 Diabetes. Diabetes Care 2016; 39(5): 823–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
