

A phase II dose-ranging study of mirabegron in patients with overactive bladder
- PMID: 23471546
- PMCID: PMC3745617
- DOI: 10.1007/s00192-013-2042-x
A phase II dose-ranging study of mirabegron in patients with overactive bladder
Abstract
Introduction and hypothesis: Mirabegron is a potent and selective β3-adrenoceptor agonist that may represent an alternative treatment option in place of antimuscarinics for patients with overactive bladder.
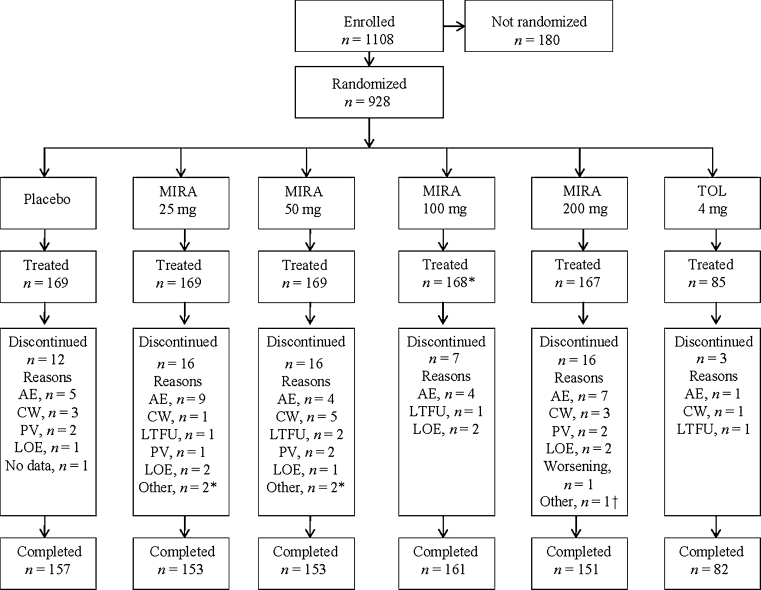
Methods: Patients completed a single-blinded, 2-week placebo run-in period followed by 12 weeks of randomized (n = 928) double-blinded treatment with mirabegron oral controlled absorption system (OCAS) 25, 50, 100, or 200 mg once-daily (QD), placebo or tolterodine extended release (ER) 4 mg QD. The primary endpoint was change from baseline to end-of-treatment in mean number of micturition episodes/24 h. Secondary endpoints included changes in mean volume voided per micturition; mean number of urinary incontinence, urgency urinary incontinence, and urgency episodes/24 h; severity of urgency; nocturia; and quality of life measures. Safety parameters included vital signs, adverse events, laboratory tests, electrocardiogram measurements and post-void residual volume.
Results: Mirabegron 25, 50, 100, and 200 mg resulted in dose-dependent reductions (improvements) from baseline to end-of-treatment in micturition frequency of 1.9, 2.1, 2.1, and 2.2 micturitions/24 h respectively, versus 1.4 micturitions/24 h with placebo (p ≤ 0.05 for the mirabegron 50-, 100-, and 200-mg comparisons). There was a statistically significant improvement with mirabegron compared with placebo for most secondary endpoints including quality of life variables. While there was a significant (p < 0.05) increase from baseline in pulse rate in the mirabegron 100-mg and 200-mg groups, this was not associated with an increased incidence of cardiovascular adverse events.
Conclusions: The favorable efficacy and tolerability of mirabegron in this phase II dose-finding study has led to its successful advancement into a phase III clinical development program.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
