

Impact of Safety-Related Dose Reductions or Discontinuations on Sustained Virologic Response in HCV-Infected Patients: Results from the GUARD-C Cohort
- PMID: 27018988
- PMCID: PMC4809570
- DOI: 10.1371/journal.pone.0151703
Impact of Safety-Related Dose Reductions or Discontinuations on Sustained Virologic Response in HCV-Infected Patients: Results from the GUARD-C Cohort
Abstract
Background: Despite the introduction of direct-acting antiviral agents for chronic hepatitis C virus (HCV) infection, peginterferon alfa/ribavirin remains relevant in many resource-constrained settings. The non-randomized GUARD-C cohort investigated baseline predictors of safety-related dose reductions or discontinuations (sr-RD) and their impact on sustained virologic response (SVR) in patients receiving peginterferon alfa/ribavirin in routine practice.
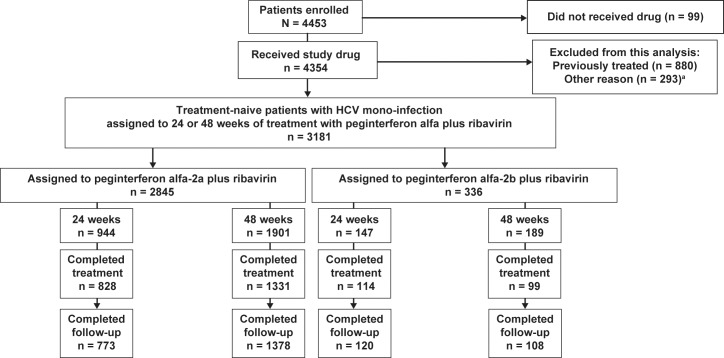
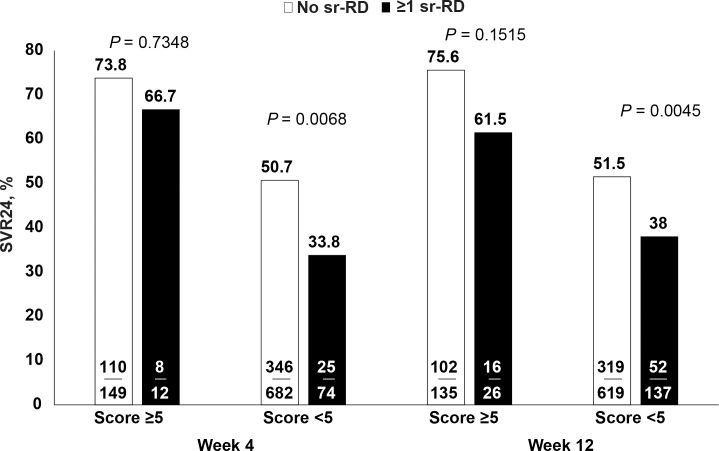
Methods: A total of 3181 HCV-mono-infected treatment-naive patients were assigned to 24 or 48 weeks of peginterferon alfa/ribavirin by their physician. Patients were categorized by time-to-first sr-RD (Week 4/12). Detailed analyses of the impact of sr-RD on SVR24 (HCV RNA <50 IU/mL) were conducted in 951 Caucasian, noncirrhotic genotype (G)1 patients assigned to peginterferon alfa-2a/ribavirin for 48 weeks. The probability of SVR24 was identified by a baseline scoring system (range: 0-9 points) on which scores of 5 to 9 and <5 represent high and low probability of SVR24, respectively.
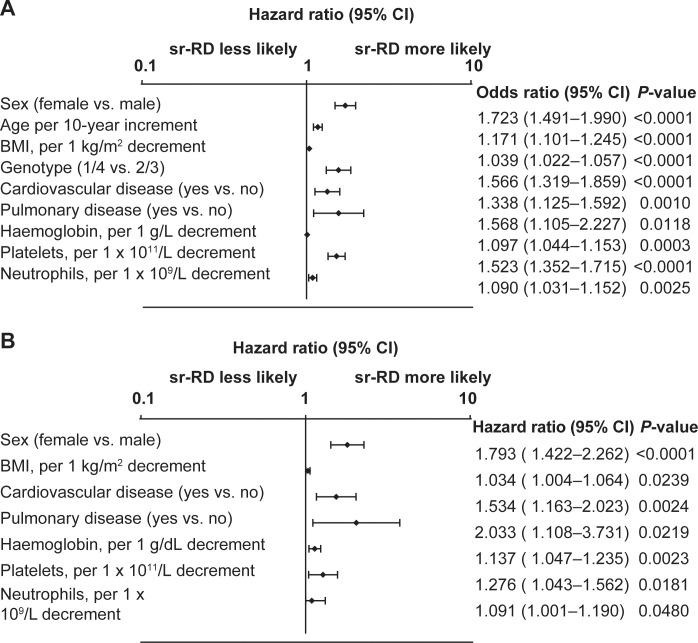
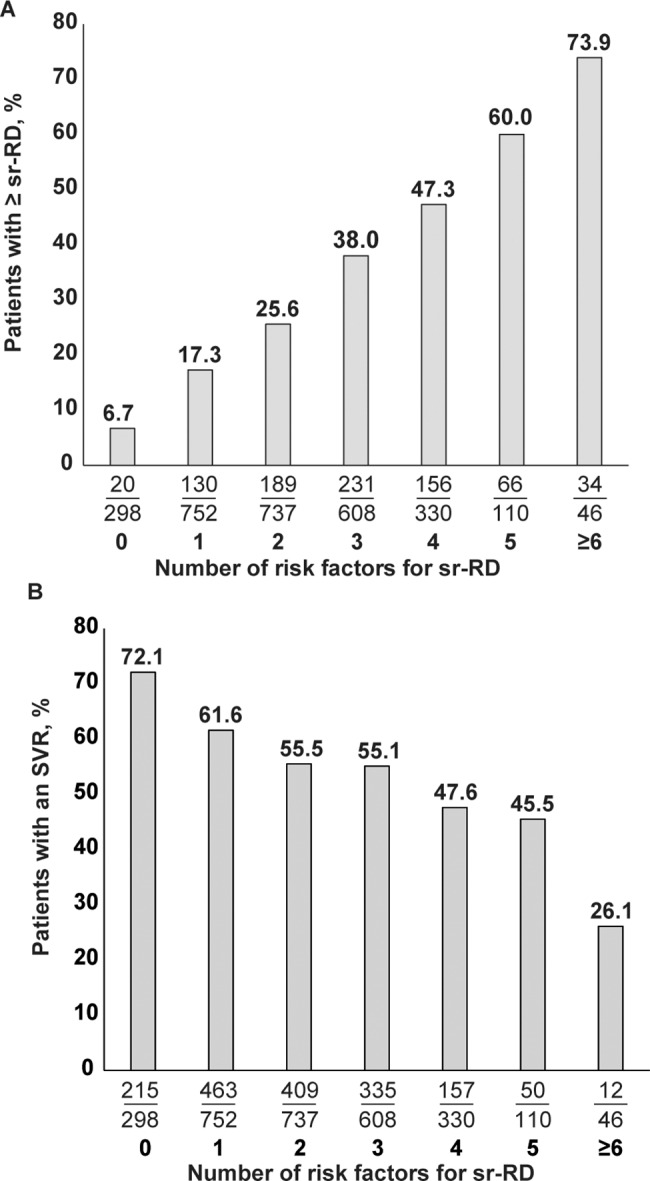
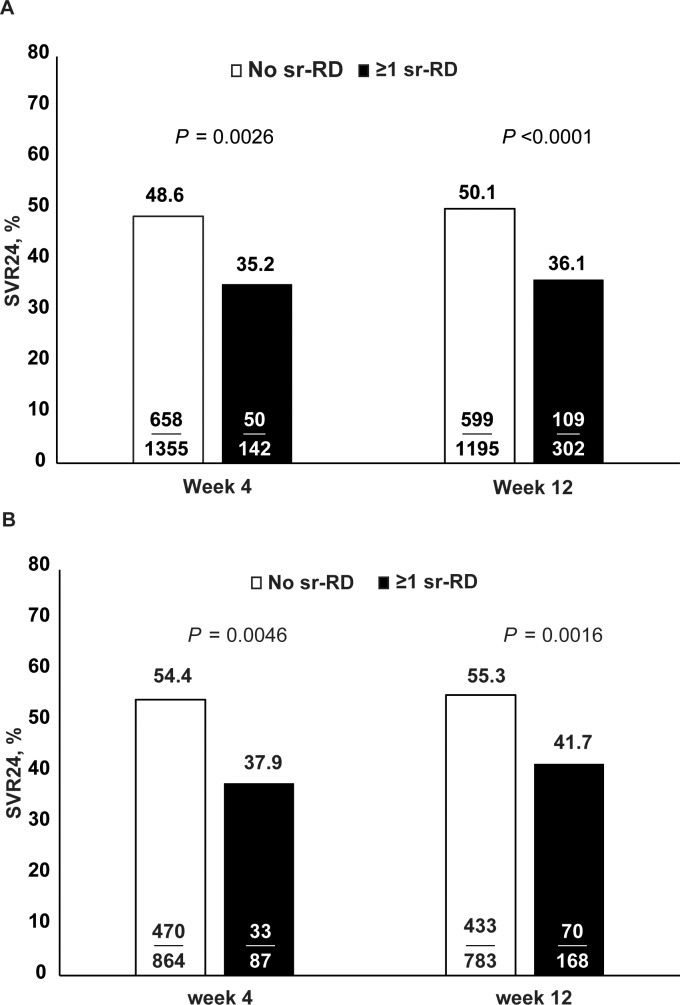
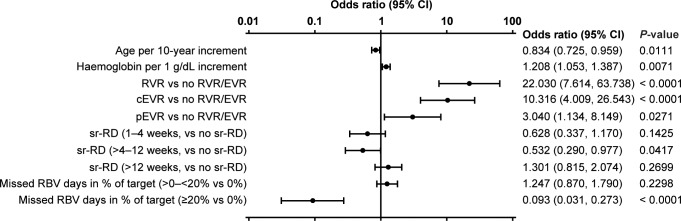
Results: SVR24 rates were 46.1% (754/1634), 77.1% (279/362), 68.0% (514/756), and 51.3% (203/396), respectively, in G1, 2, 3, and 4 patients. Overall, 16.9% and 21.8% patients experienced ≥1 sr-RD for peginterferon alfa and ribavirin, respectively. Among Caucasian noncirrhotic G1 patients: female sex, lower body mass index, pre-existing cardiovascular/pulmonary disease, and low hematological indices were prognostic factors of sr-RD; SVR24 was lower in patients with ≥1 vs. no sr-RD by Week 4 (37.9% vs. 54.4%; P = 0.0046) and Week 12 (41.7% vs. 55.3%; P = 0.0016); sr-RD by Week 4/12 significantly reduced SVR24 in patients with scores <5 but not ≥5.
Conclusions: In conclusion, sr-RD to peginterferon alfa-2a/ribavirin significantly impacts on SVR24 rates in treatment-naive G1 noncirrhotic Caucasian patients. Baseline characteristics can help select patients with a high probability of SVR24 and a low probability of sr-RD with peginterferon alfa-2a/ribavirin.
Trial registration: ClinicalTrials.gov NCT01344889.
Conflict of interest statement
Figures
References
-
- American Association for the Study of Liver Diseases and Infectious Diseases Society of America. Recommendations for testing, managing, and treating hepatitis C. Available: http://www.hcvguidelines.org. Accessed 24 Aug 2014. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
