

Community-Acquired Pneumonia in the Immunocompromised Host: Epidemiology and Outcomes
- PMID: 38023559
- PMCID: PMC10676121
- DOI: 10.1093/ofid/ofad565
Community-Acquired Pneumonia in the Immunocompromised Host: Epidemiology and Outcomes
Abstract
Background: The epidemiology and outcomes of community-acquired pneumonia (CAP) in immunocompromised hosts (ICHs) are not well defined. The objective of this study was to define the epidemiology and outcomes of CAP in ICHs as compared with non-ICHs.
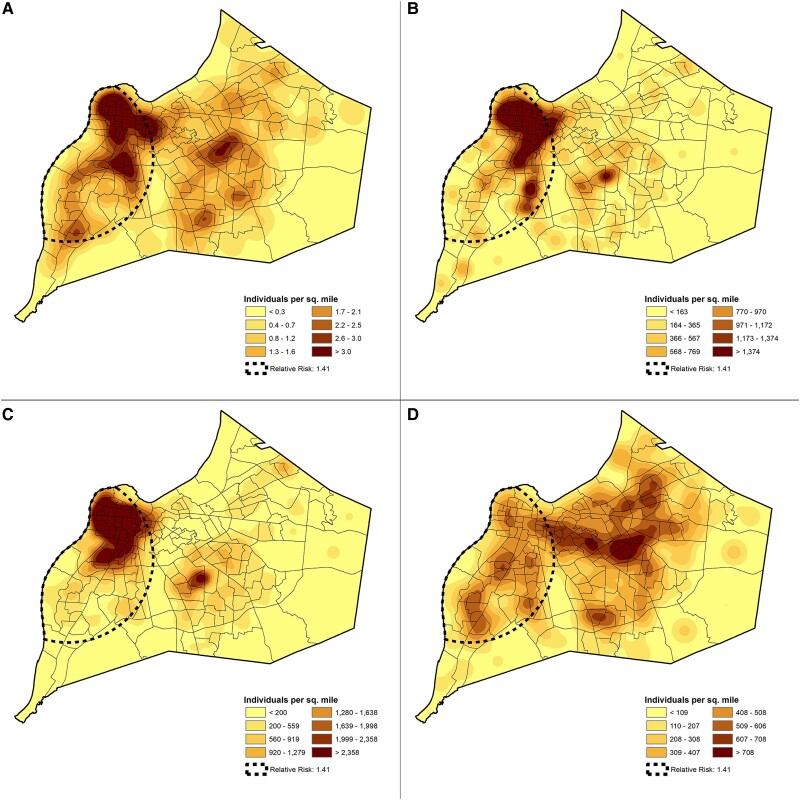
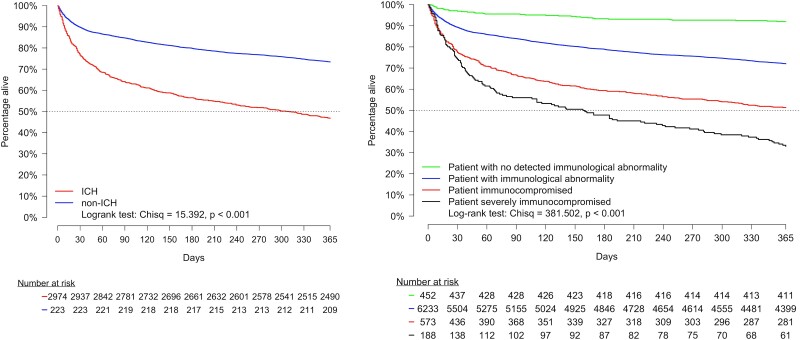
Methods: This ancillary study included a prospective cohort of hospitalized adult Louisville residents with CAP from 1 June 2014 to 31 May 2016. An ICH was defined per the criteria of the Centers for Disease Control and Prevention. Geospatial epidemiology explored associations between ICHs hospitalized with CAP and income level, race, and age. Mortality for ICHs and non-ICHs was evaluated during hospitalization and 30 days, 6 months, and 1 year after hospitalization.
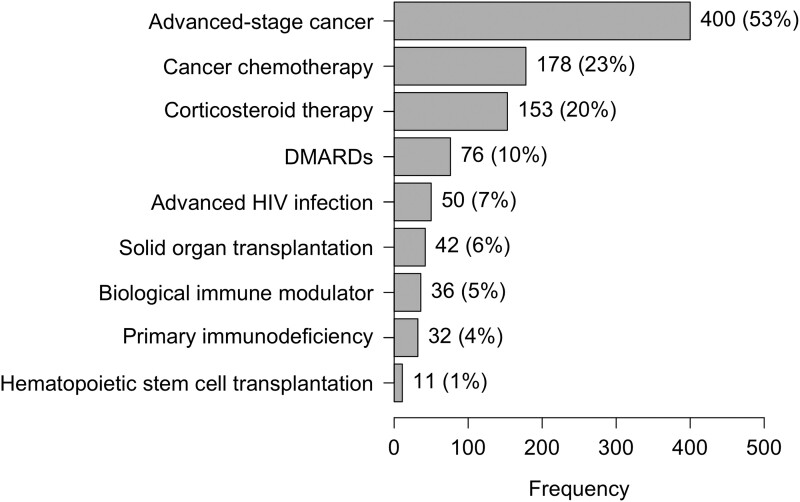
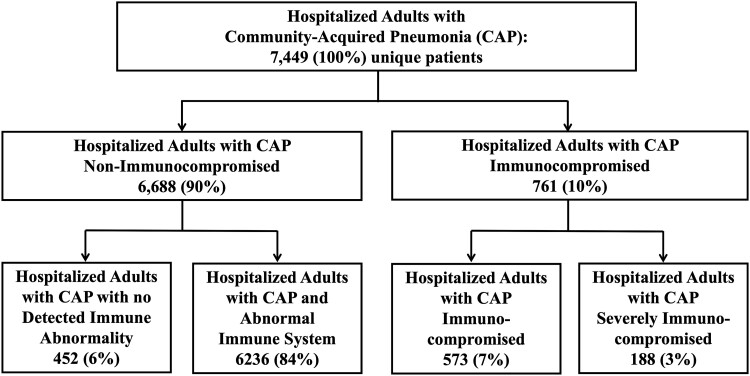
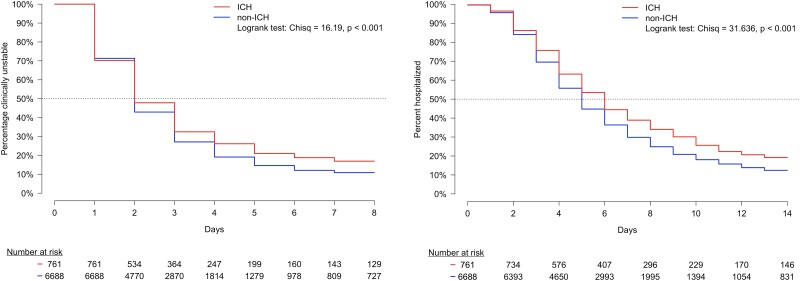
Results: A total of 761 (10%) ICHs were identified among 7449 patients hospitalized with CAP. The most common immunocompromising medical conditions or treatments were advanced-stage cancer (53%), cancer chemotherapy (23%), and corticosteroid use (20%). Clusters of ICHs hospitalized with CAP were found in areas associated with low-income and Black or African American populations. Mortality by time point for ICHs vs non-ICHs was as follows: hospitalization, 9% vs 5%; 30 days, 24% vs 11%; 6 months, 44% vs 21%; and 1 year, 53% vs 27%, respectively.
Conclusions: Approximately 1 in 10 hospitalized patients with CAP is immunocompromised, with advanced-stage cancer being the most frequent immunocompromising condition, as seen in half of all patients who are immunocompromised. Risk for hospitalization may be influenced by socioeconomic disparities and/or race. ICHs have a 2-fold increase in mortality as compared with non-ICHs.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Harpaz R, Dahl RM, Dooling KL. Prevalence of immunosuppression among US adults, 2013. JAMA 2016; 316:2547–8. - PubMed
-
- Jenkinson PW, Plevris N, Siakavellas S, et al. Temporal trends in surgical resection rates and biologic prescribing in Crohn’s disease: a population-based cohort study. J Crohns Colitis 2020; 14:1241–7. - PubMed
-
- Organ Procurement and Transplantation Network . National data: transplants in the US by region. Available at: https://optn.transplant.hrsa.gov/data/view-datareports/national-data/#. Accessed 7 July 2023.
-
- Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. Natl Vital Stat Rep 2016; 64:1–119. - PubMed
-
- Pfuntner A, Wier LM, Stocks C. Most Frequent Conditions in US Hospitals, 2011. Rockville: Agency for Healthcare Research and Quality, 2013. Healthcare Cost and Utilization Project statistical brief 162.
LinkOut - more resources
Full Text Sources
Miscellaneous
