

Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies
- PMID: 29676281
- PMCID: PMC5899998
- DOI: 10.1016/S0140-6736(18)30134-X
Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies
Erratum in
-
Department of Error.Lancet. 2018 Jun 2;391(10136):2212. doi: 10.1016/S0140-6736(18)31168-1. Epub 2018 Jun 1. Lancet. 2018. PMID: 29893221 Free PMC article. No abstract available.
Abstract
Background: Low-risk limits recommended for alcohol consumption vary substantially across different national guidelines. To define thresholds associated with lowest risk for all-cause mortality and cardiovascular disease, we studied individual-participant data from 599 912 current drinkers without previous cardiovascular disease.
Methods: We did a combined analysis of individual-participant data from three large-scale data sources in 19 high-income countries (the Emerging Risk Factors Collaboration, EPIC-CVD, and the UK Biobank). We characterised dose-response associations and calculated hazard ratios (HRs) per 100 g per week of alcohol (12·5 units per week) across 83 prospective studies, adjusting at least for study or centre, age, sex, smoking, and diabetes. To be eligible for the analysis, participants had to have information recorded about their alcohol consumption amount and status (ie, non-drinker vs current drinker), plus age, sex, history of diabetes and smoking status, at least 1 year of follow-up after baseline, and no baseline history of cardiovascular disease. The main analyses focused on current drinkers, whose baseline alcohol consumption was categorised into eight predefined groups according to the amount in grams consumed per week. We assessed alcohol consumption in relation to all-cause mortality, total cardiovascular disease, and several cardiovascular disease subtypes. We corrected HRs for estimated long-term variability in alcohol consumption using 152 640 serial alcohol assessments obtained some years apart (median interval 5·6 years [5th-95th percentile 1·04-13·5]) from 71 011 participants from 37 studies.
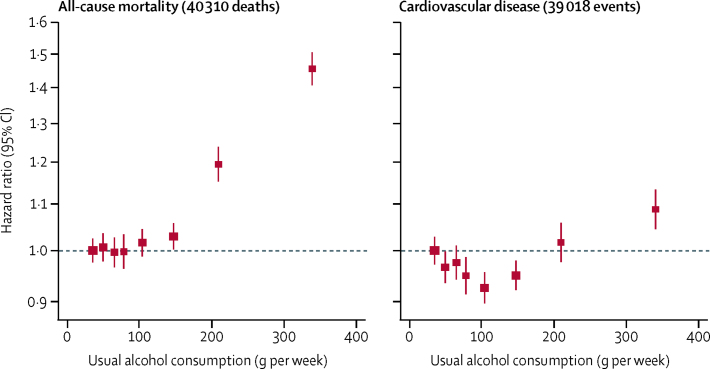
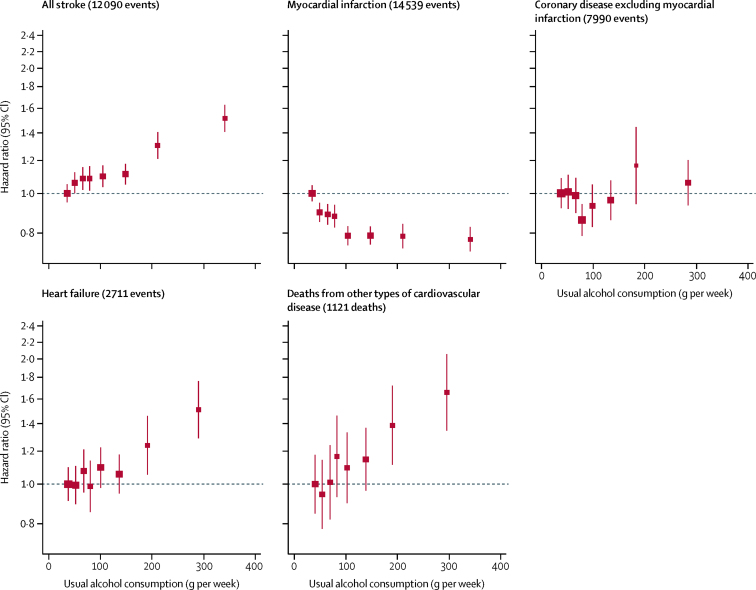
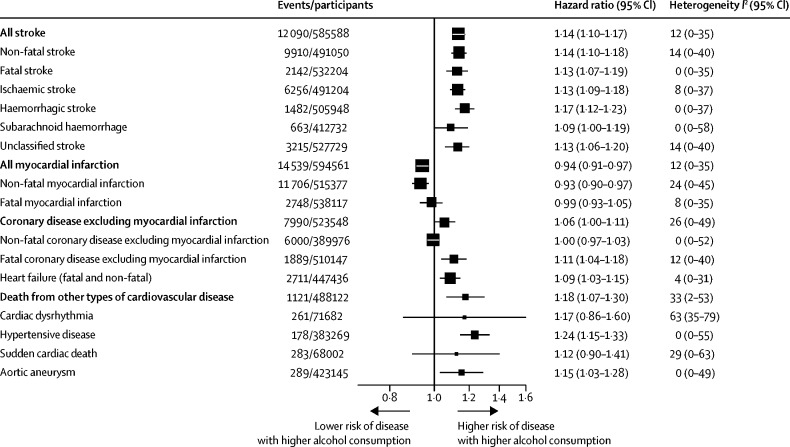
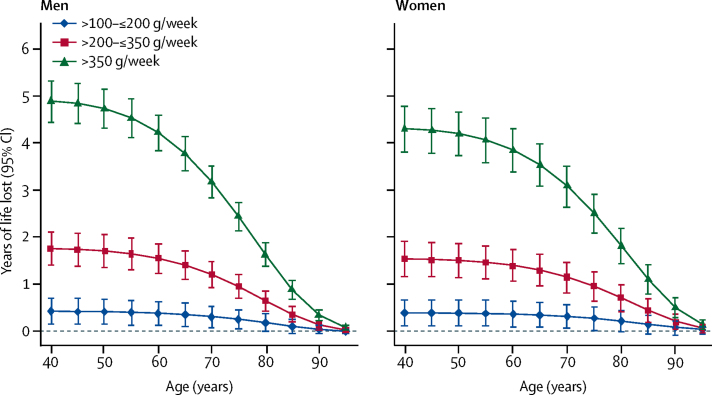
Findings: In the 599 912 current drinkers included in the analysis, we recorded 40 310 deaths and 39 018 incident cardiovascular disease events during 5·4 million person-years of follow-up. For all-cause mortality, we recorded a positive and curvilinear association with the level of alcohol consumption, with the minimum mortality risk around or below 100 g per week. Alcohol consumption was roughly linearly associated with a higher risk of stroke (HR per 100 g per week higher consumption 1·14, 95% CI, 1·10-1·17), coronary disease excluding myocardial infarction (1·06, 1·00-1·11), heart failure (1·09, 1·03-1·15), fatal hypertensive disease (1·24, 1·15-1·33); and fatal aortic aneurysm (1·15, 1·03-1·28). By contrast, increased alcohol consumption was log-linearly associated with a lower risk of myocardial infarction (HR 0·94, 0·91-0·97). In comparison to those who reported drinking >0-≤100 g per week, those who reported drinking >100-≤200 g per week, >200-≤350 g per week, or >350 g per week had lower life expectancy at age 40 years of approximately 6 months, 1-2 years, or 4-5 years, respectively.
Interpretation: In current drinkers of alcohol in high-income countries, the threshold for lowest risk of all-cause mortality was about 100 g/week. For cardiovascular disease subtypes other than myocardial infarction, there were no clear risk thresholds below which lower alcohol consumption stopped being associated with lower disease risk. These data support limits for alcohol consumption that are lower than those recommended in most current guidelines.
Funding: UK Medical Research Council, British Heart Foundation, National Institute for Health Research, European Union Framework 7, and European Research Council.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Thresholds for safer alcohol use might need lowering.Lancet. 2018 Apr 14;391(10129):1460-1461. doi: 10.1016/S0140-6736(18)30545-2. Lancet. 2018. PMID: 29676264 No abstract available.
-
Consuming 100 g/week or less of alcohol was associated with the lowest risk of all-cause mortality.BMJ Evid Based Med. 2019 Jun;24(3):117-118. doi: 10.1136/bmjebm-2018-111049. Epub 2018 Sep 3. BMJ Evid Based Med. 2019. PMID: 30177544 No abstract available.
-
Risk thresholds for alcohol consumption.Lancet. 2018 Nov 17;392(10160):2165-2166. doi: 10.1016/S0140-6736(18)32192-5. Lancet. 2018. PMID: 30496094 No abstract available.
-
Risk thresholds for alcohol consumption.Lancet. 2018 Nov 17;392(10160):2166-2167. doi: 10.1016/S0140-6736(18)32202-5. Lancet. 2018. PMID: 30496095 No abstract available.
-
Risk thresholds for alcohol consumption.Lancet. 2018 Nov 17;392(10160):2167. doi: 10.1016/S0140-6736(18)32197-4. Lancet. 2018. PMID: 30496097 No abstract available.
References
-
- Department of Health Alcohol Guidelines Review: Report from the guidelines development group to the UK Chief Medical Officers. 2016. https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil... (accessed Feb 5, 2018).
-
- Kalinowski A, Humphreys K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction. 2016;111:1293–1298. - PubMed
-
- Stampfer MJ, Colditz GA, Willett WC, Speizer FE, Hennekens CH. A prospective study of moderate alcohol consumption and the risk of coronary disease and stroke in women. N Engl J Med. 1988;319:267–273. - PubMed
-
- Boffetta P, Garfinkel L. Alcohol drinking and mortality among men enrolled in an American Cancer Society prospective study. Epidemiology. 1990;1:342–348. - PubMed
-
- Thun MJ, Peto R, Lopez AD. Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med. 1997;337:1705–1714. - PubMed
Publication types
MeSH terms
Grants and funding
- MR/R024227/1/MRC_/Medical Research Council/United Kingdom
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- U10 AA025286/AA/NIAAA NIH HHS/United States
- 268834/ERC_/European Research Council/International
- CH/12/2/29428/BHF_/British Heart Foundation/United Kingdom
- G0701619/MRC_/Medical Research Council/United Kingdom
- MC_UU_12015/5/MRC_/Medical Research Council/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- G0700463/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- G0800270/MRC_/Medical Research Council/United Kingdom
- 16491/CRUK_/Cancer Research UK/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- NC/P001076/1/NC3RS_/National Centre for the Replacement, Refinement and Reduction of Animals in Research/United Kingdom
- MC_UU_12012/5/MRC_/Medical Research Council/United Kingdom
- MC_UU_12015/1/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_UU_00002/7/MRC_/Medical Research Council/United Kingdom
- RG/16/11/32334/BHF_/British Heart Foundation/United Kingdom
- MR/K013351/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- 204623/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 001/WHO_/World Health Organization/International
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MR/K014811/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
