

Risk factors for ANA positivity in healthy persons
- PMID: 21366908
- PMCID: PMC3132017
- DOI: 10.1186/ar3271
Risk factors for ANA positivity in healthy persons
Abstract
Introduction: The finding of antinuclear antibody (ANA) positivity in a healthy individual is usually of unknown significance and in most cases is benign. However, a subset of such individuals is at risk for development of autoimmune disease. We examined demographic and immunological features that are associated with ANA positivity in clinically healthy persons to develop insights into when this marker carries risk of progression to lupus.
Methods: Biological samples from healthy individuals and patients with systemic lupus erythematosus (SLE) were obtained from the Dallas Regional Autoimmune Disease Registry (DRADR). Measurements carried out on serum samples included ANA, extractable nuclear antibodies (ENA) and autoantibody profiling using an array with more than 100 specificities. Whole blood RNA samples from a subset of individuals were used to analyze gene expression on the Illumina platform. Data were analyzed for associations of high ANA levels with demographic features, the presence of other autoantibodies and with gene expression profiles.
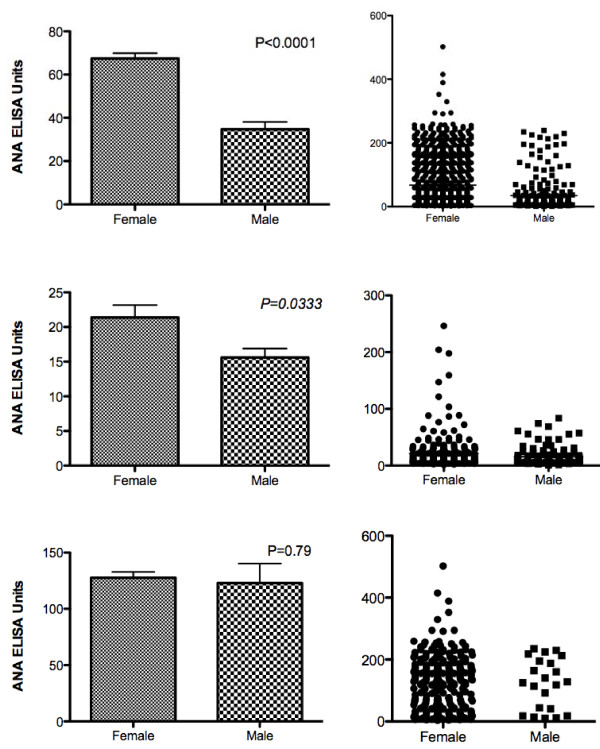
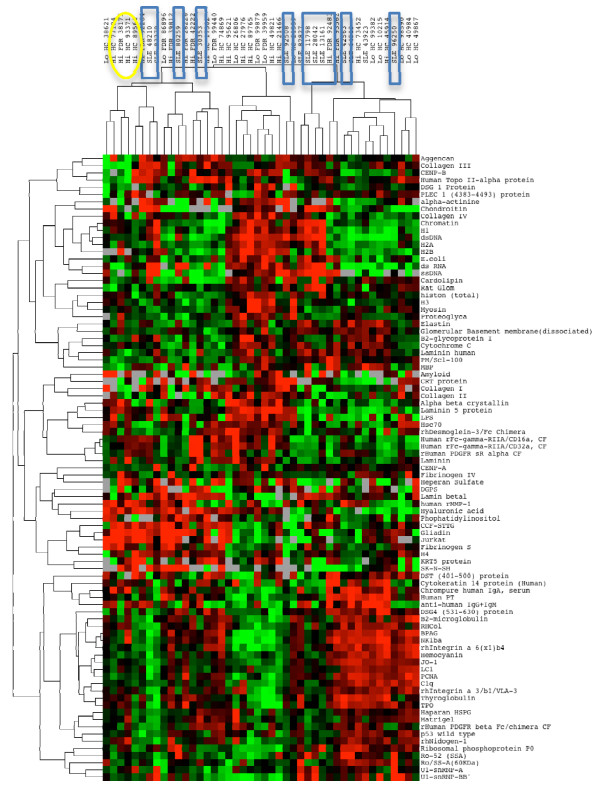
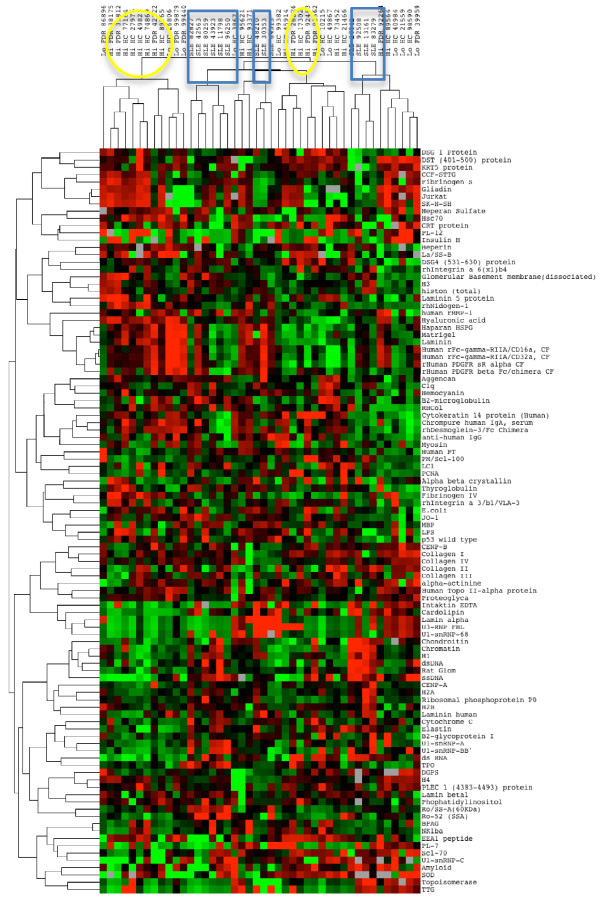
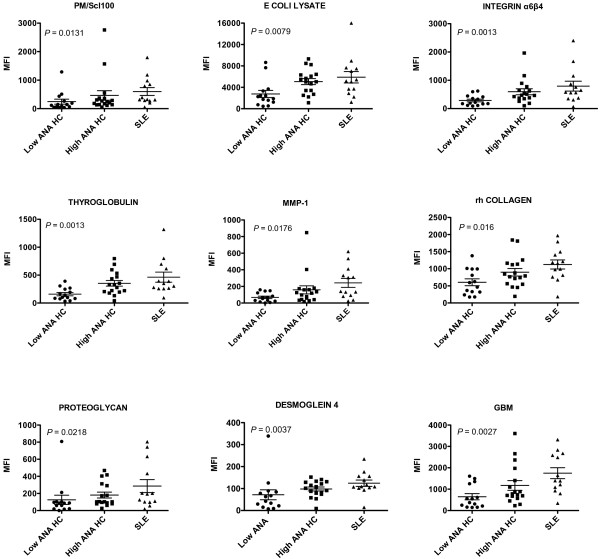
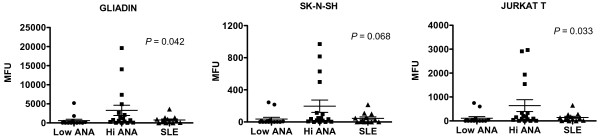
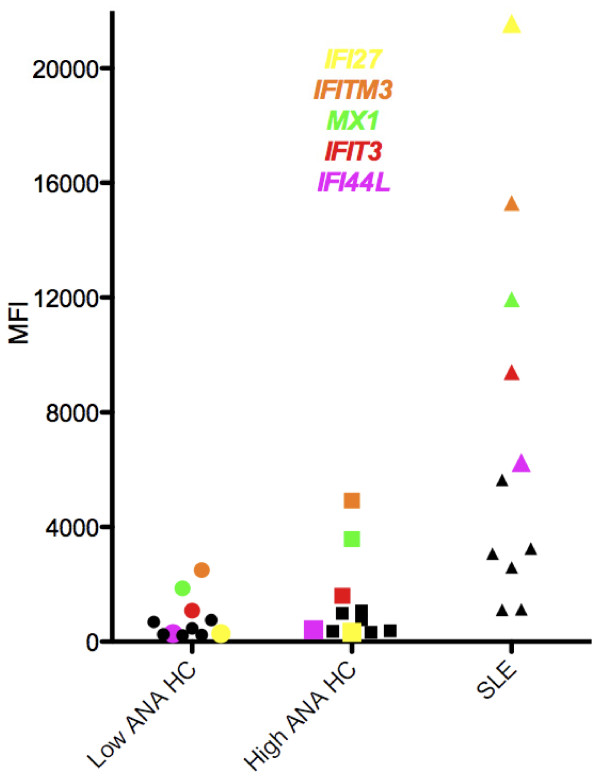
Results: Overall, ANA levels are significantly higher in females than in males and this association holds in patients with the autoimmune diseases lupus and rheumatoid arthritis (RA) as well as in healthy controls (HC). Age was not significantly associated with ANA levels and the elevated ANA values could not be explained by higher IgG levels. Another autoantibody, anti- cyclic citrullinated peptide (CCP), did not show gender dimorphism in rheumatoid arthritis (RA) or healthy individuals. The autoantigen array showed significant elevations of other autoantibodies in high ANA HCs. Some of these autoantibodies were directed to antigens in skin and others were related to autoimmune conditions of kidney, thyroid or joints. Gene expression analyses showed a greater prevalence of significantly upregulated genes in HCs with negative ANA values than in those with significant ANA positivity. Genes upregulated in high ANA HCs included a celiac disease autoantigen and some components of the Type I interferon (IFN) gene signature.
Conclusions: Risks for ANA positivity include female gender and organ-specific autoimmunity. Upregulation of skin-specific autoantibodies may indicate that early events in the break of tolerance take place in cutaneous structures. Some of these changes may be mediated by Type I IFN. Blood profiling for expressed autoantibodies and genes has the potential to identify individuals at risk for development of autoimmune diseases including lupus.
Figures

Comment in
-
Antinuclear antibodies in healthy people: the tip of autoimmunity's iceberg?Arthritis Res Ther. 2011 Apr 21;13(2):109. doi: 10.1186/ar3282. Arthritis Res Ther. 2011. PMID: 21554754 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
